NEET-PG 2022 — Anatomy
9 Previous Year Questions with Answers & Explanations
Altered sensation over the area of the great saphenous vein in the leg is seen due to an injury to which of the following nerves?
A 50-year-old man with carcinoma of the prostate presents with X-ray findings showing sclerosis and collapse of T10 and T11 vertebrae. The spread of cancer to these vertebrae most probably occurred through which route?
Identify the type of cartilage shown in the image.
The structure marked A in the image below gives rise to which of the following structures?
A patient presents with an anesthetic patch in areas of the face. Which of the following nerves is the most commonly involved in this condition?
A patient presents with the complaint of inability to close the eye, drooling of saliva, and deviation of the angle of the mouth. Which of the following nerves is most likely to be affected?
A 70-year-old male patient presents with high-frequency hearing loss. It was noted that the basilar membrane was affected. Which of the following structures lies near the affected structure?
The given histology image is of which structure?
Among the following the plane of least pelvic dimension is:
NEET-PG 2022 - Anatomy NEET-PG Practice Questions and MCQs
Question 1: Altered sensation over the area of the great saphenous vein in the leg is seen due to an injury to which of the following nerves?
- A. Fibular
- B. Femoral (Correct Answer)
- C. Tibial
- D. Sural
Explanation: ***Femoral*** - The **femoral nerve** gives rise to the **saphenous nerve**, which runs with the great saphenous vein and provides sensation to the medial aspect of the leg and foot. - Injury to the femoral nerve or its saphenous branch can result in altered sensation in the distribution of the **great saphenous vein**. *Tibial* - The **tibial nerve** innervates muscles in the posterior compartment of the leg and provides sensation to the sole of the foot and parts of the ankle, not the area of the great saphenous vein. - Injury to the tibial nerve often leads to **motor deficits** (plantar flexion) and sensory loss on the bottom of the foot. *Sural* - The **sural nerve** provides sensation to the posterolateral aspect of the leg and the lateral side of the foot, distinct from the great saphenous vein's territory. - This nerve is often injured during procedures around the **lateral malleolus** or Achilles tendon. *Fibular* - The **fibular nerve** (also known as the common peroneal nerve) innervates the anterior and lateral compartments of the leg and provides sensation to the dorsum of the foot and lateral leg. - Injury typically results in **foot drop** and sensory loss **dorsum of foot**.
Question 2: A 50-year-old man with carcinoma of the prostate presents with X-ray findings showing sclerosis and collapse of T10 and T11 vertebrae. The spread of cancer to these vertebrae most probably occurred through which route?
- A. Internal vertebral plexus of veins (Batson's plexus) (Correct Answer)
- B. Spread through the sacral canal to the vertebrae
- C. Spread via superior rectal veins to the vertebrae
- D. Spread through lymphatic vessels to the vertebrae
Explanation: ***Internal vertebral plexus of veins (Batson's plexus)*** - The **Batson's plexus** is a valveless network of veins directly connecting the pelvic venous plexuses (including those draining the prostate) with the vertebral venous system. - This valveless nature allows for easy retrograde flow of tumor cells, especially during increases in intra-abdominal pressure (e.g., coughing, straining), facilitating direct spread from the prostate to the vertebrae. *Spread through the sacral canal to the vertebrae* - While the sacral canal contains structures, it is a bony canal and not a primary route for direct hematogenous or lymphatic metastatic spread of prostate cancer to the vertebral bodies. - Metastasis through the sacral canal itself would typically imply direct extension or invasion, which is less common for widespread vertebral metastases than venous dissemination. *Spread via superior rectal veins to the vertebrae* - The **superior rectal veins** drain into the inferior mesenteric vein, which is part of the portal system, eventually leading to the hepatic circulation. - While this route can lead to liver metastases, it generally does not directly connect to the vertebral venous system in a way that would explain isolated vertebral metastases without liver involvement. *Spread through lymphatic vessels to the vertebrae* - Lymphatic spread from prostate cancer typically involves regional **pelvic lymph nodes** first (e.g., obturator, internal iliac, presacral). - While lymphatic spread can occur, it usually precedes or accompanies distant metastases and is less likely to be the sole, direct route for vertebral involvement without evident lymphadenopathy in the direct path.
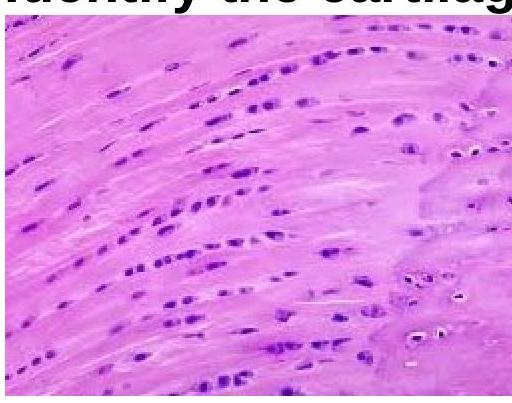
Question 3: Identify the type of cartilage shown in the image.
- A. Hyaline cartilage
- B. Elastic cartilage
- C. Dense connective tissue
- D. Fibrocartilage (Correct Answer)
Explanation: ***Fibrocartilage*** - The image displays **chondrocytes** arranged in rows between bundles of **collagen fibers**, characteristic of fibrocartilage. This structure provides high tensile strength and shock absorption. - Unlike other cartilage types, fibrocartilage lacks a distinct perichondrium and is found in structures requiring extreme strength, such as intervertebral discs and menisci. *Hyaline cartilage* - Hyaline cartilage has an amorphous, **glassy matrix** with chondrocytes typically arranged in small groups (isogenous groups) within lacunae, without prominent collagen bundles. - It is found in articular surfaces, tracheal rings, and the costal cartilages, providing smooth, low-friction surfaces. *Elastic cartilage* - Elastic cartilage is characterized by a high concentration of **elastic fibers** within its matrix, giving it flexibility and resilience. - Chondrocytes are typically scattered and the matrix stains darker due to the elastic fibers, which are not apparent in the image. *Dense connective tissue* - While dense connective tissue contains abundant **collagen fibers**, it lacks chondrocytes in lacunae, instead containing fibroblasts. - The presence of chondrocytes in the image confirms this is cartilage, not dense connective tissue.
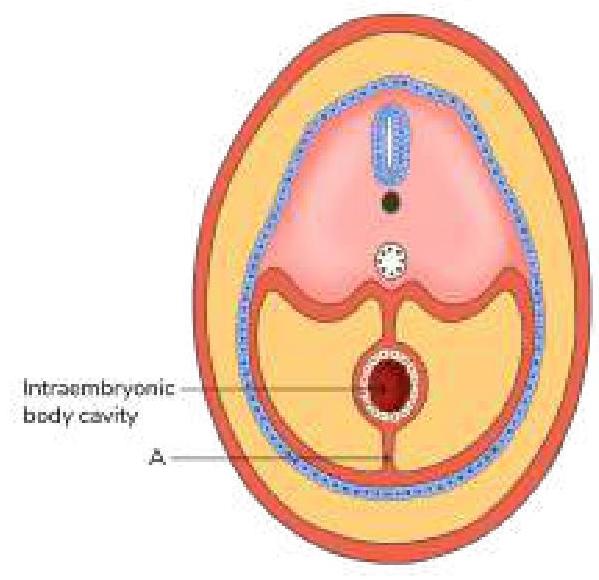
Question 4: The structure marked A in the image below gives rise to which of the following structures?
- A. Lienorenal ligament
- B. Gastrophrenic ligament
- C. Gastrosplenic ligament
- D. Falciform ligament (Correct Answer)
Explanation: ***Falciform ligament*** - The structure marked 'A' represents the **ventral mesentery** in the embryonic stage, which connects the primitive gut tube to the anterior body wall. - The **falciform ligament** develops from the ventral mesentery, specifically in the region of the liver, and connects the liver to the anterior abdominal wall and diaphragm. *Gastrosplenic ligament* - This ligament is derived from the **dorsal mesentery**, not the ventral mesentery. - It connects the greater curvature of the stomach to the hilum of the spleen. *Lienorenal ligament* - Also derived from the **dorsal mesentery**, connecting the left kidney to the spleen. - This structure is not formed from the ventral mesentery which is indicated by 'A'. *Gastrophrenic ligament* - This ligament is part of the **dorsal mesentery** and connects the stomach to the diaphragm. - It is not a derivative of the ventral mesentery.
Question 5: A patient presents with an anesthetic patch in areas of the face. Which of the following nerves is the most commonly involved in this condition?
- A. Facial nerve
- B. Abducens nerve
- C. Trigeminal nerve (Correct Answer)
- D. Optic nerve
Explanation: ***Trigeminal nerve*** - The **trigeminal nerve** (CN V) is responsible for **sensory innervation of the face, scalp, and mucous membranes** of the mouth and nose [1]. An anesthetic patch suggests a loss of sensation in these areas. - Involvement of the trigeminal nerve, particularly its branches (ophthalmic, maxillary, mandibular), would lead to **paresthesia, numbness, or anesthesia** in the corresponding dermatomes of the face. *Abducens nerve* - The **abducens nerve** (CN VI) primarily controls the **lateral rectus muscle**, responsible for **abduction of the eye**. - Dysfunction of this nerve would lead to **diplopia (double vision)** and an inability to move the eye laterally, not facial anesthesia. *Facial nerve* - The **facial nerve** (CN VII) is mainly responsible for **motor innervation of the muscles of facial expression** and taste from the anterior two-thirds of the tongue. - Damage to this nerve causes **facial weakness or paralysis** (e.g., Bell's palsy) and taste disturbances, not loss of sensation (anesthesia) in facial skin. *Optic nerve* - The **optic nerve** (CN II) is solely responsible for **vision**. - Damage to the optic nerve results in **visual field defects or blindness**, not sensory changes on the face.
Question 6: A patient presents with the complaint of inability to close the eye, drooling of saliva, and deviation of the angle of the mouth. Which of the following nerves is most likely to be affected?
- A. Facial nerve (Correct Answer)
- B. Trigeminal nerve
- C. Oculomotor nerve
- D. Glossopharyngeal nerve
Explanation: ***Facial nerve*** - The **facial nerve (cranial nerve VII)** controls the muscles of facial expression, including those for eye closure and mouth movement. - Damage to the facial nerve leads to **unilateral facial weakness or paralysis**, causing inability to close the eye, drooling from the corner of the mouth, and deviation of the mouth. *Trigeminal nerve* - The **trigeminal nerve (cranial nerve V)** is primarily responsible for **facial sensation** and **mastication (chewing)**. - Dysfunction typically presents as facial numbness, pain, or difficulty chewing, not facial muscle paralysis. *Oculomotor nerve* - The **oculomotor nerve (cranial nerve III)** controls most **extraocular muscles** (eye movements), pupillary constriction, and lifts the eyelid. - Damage would result in ptosis (drooping eyelid), dilated pupil, and outward and downward deviation of the eye. *Glossopharyngeal nerve* - The **glossopharyngeal nerve (cranial nerve IX)** is involved in **taste from the posterior tongue**, **swallowing**, and sensation from the pharynx. - Its impairment can lead to difficulty swallowing, loss of gag reflex, or altered taste, but not facial paralysis.
Question 7: A 70-year-old male patient presents with high-frequency hearing loss. It was noted that the basilar membrane was affected. Which of the following structures lies near the affected structure?
- A. Stria vascularis (Correct Answer)
- B. Modiolus
- C. Helicotrema
- D. Oval window
Explanation: ***Stria vascularis*** - The **stria vascularis** is a highly vascularized epithelial layer located on the lateral wall of the **scala media**, directly adjacent to the **basilar membrane**. - It is crucial for maintaining the high potassium concentration in the **endolymph** which is essential for the function of hair cells in the **organ of Corti** and thus hearing [2]. *Modiolus* - The **modiolus** is the central, conical bony pillar of the cochlea, around which the cochlear duct spirals. - While it houses the **spiral ganglion** and auditory nerve fibers, it is structurally distinct from and not immediately adjacent to the basilar membrane. *Helicotrema* - The **helicotrema** is the small opening at the apex of the cochlea where the **scala vestibuli** and **scala tympani** communicate [1]. - It is located at the very end of the cochlea, far from the main vibratory portion of the basilar membrane responsible for high-frequency sounds. *Oval window* - The **oval window** is the opening in the bony labyrinth into which the **stapes** footplate fits, transmitting vibrations from the middle ear to the inner ear [2]. - While critical for hearing, it is located at the base of the cochlea and is not an immediate neighbor of the basilar membrane in the context of its function in sound transduction within the cochlear duct.
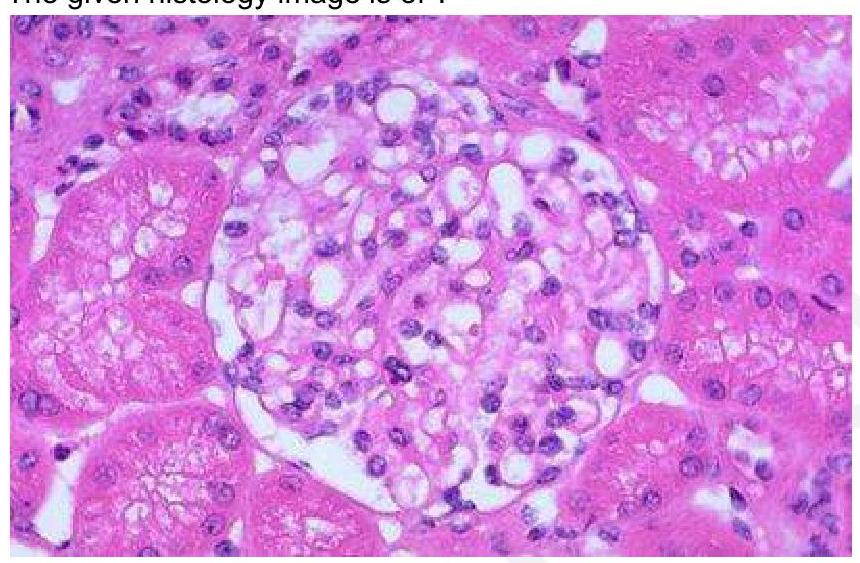
Question 8: The given histology image is of which structure?
- A. Pancreatic islet cells
- B. Hassall's corpuscles
- C. Glomerulus (Correct Answer)
- D. Leydig cells in the testis
Explanation: ***Glomerulus*** - The glomerulus is characterized by a **tuft of capillaries** surrounded by Bowman's capsule, responsible for filtration in the kidney [1]. - Histological examination typically shows a **dense network of capillaries** and **mesangial cells**, which are distinct features of the glomeruli [1]. *Hassall's corpuscles* - Found in the **thymus**, they are round structures composed of epithelial cells, crucial in T-cell maturation. - Histologically, they present as concentric layers of **epithelial cells** and are not found in the kidney. *Leydig cells of testis* - Located in the **interstitial tissue** of the testes, these cells produce testosterone and are typically larger than glomerular cells. - They are characterized by their **eosinophilic cytoplasm** and round nuclei, differing markedly from the structures found in the glomerulus. *Pancreatic islet cells* - Islet cells are involved in **hormone production**, predominantly insulin and glucagon, and are located in the pancreas. - Histologically, they appear as small clusters dispersed among **exocrine pancreas**, which is different from the highly organized structure of the glomerulus. **References:** [1] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Diseases Of The Urinary And Male Genital Tracts, pp. 522-523.
Question 9: Among the following the plane of least pelvic dimension is:
- A. Inlet
- B. False pelvis
- C. Mid-cavity (Correct Answer)
- D. Outlet
Explanation: ***Mid-cavity*** - The **mid-cavity** or **mid-pelvis** is the plane of smallest dimensions during labor, defined by the ischial spines laterally [1]. - This plane is crucial for determining if a fetus can successfully navigate the birth canal, as it represents the narrowest point [1]. *Inlet* - The **pelvic inlet** is the widest part of the pelvis and usually poses less of a restriction during the descent of the fetal head [1]. - It is bounded by the sacral promontory, arcuate line, pectineal line, and pubic crest [2]. *False pelvis* - The **false pelvis** is the upper, broader part of the pelvis and does not play a direct role in guiding the fetal head through the birth canal [1]. - Its boundaries are largely abdominal and do not define crucial dimensions for passage [2]. *Outlet* - The **pelvic outlet** is the final opening that the fetal head must pass through, and while its dimensions are important, the mid-cavity is generally the narrowest point. - Its dimensions are measured from the pubic arch to the tip of the coccyx [3].