All SubjectsAnatomy (18)Anesthesiology (4)Biochemistry (26)Community Medicine (33)Dental (2)Dermatology (7)ENT (7)Forensic Medicine (13)Internal Medicine (54)Microbiology (21)Obstetrics and Gynecology (28)Ophthalmology (8)Orthopaedics (5)Pathology (25)Pediatrics (18)Pharmacology (27)Physiology (21)Psychiatry (9)Radiology (17)Surgery (23)
Q11
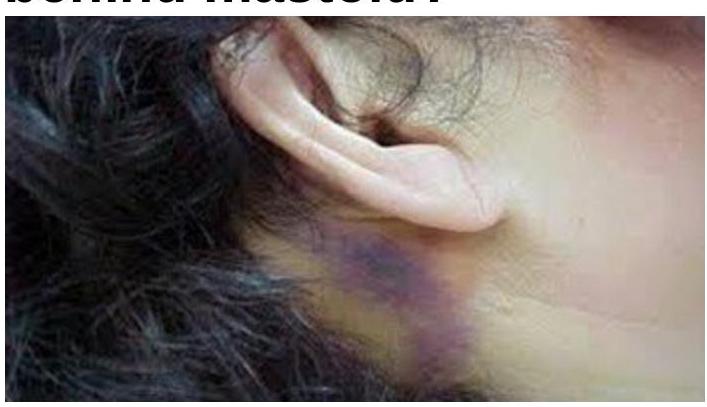
What does a bluish-purple discoloration behind the mastoid indicate?
Q12
Not a landmark of facial nerve identification in parotid surgery:
Q13
A patient presents with abdominal pain, blood in stools and a palpable mass on examination. A Barium Study was performed, probable diagnosis is?

Q14
What is the most probable cause of this condition?

Q15
Which one of the following is not a component of THORACOSCORE?
Q16
A patient is on follow-up for recurrent abdominal pain. USG reveals an aortic aneurysm of 40 mm. What should be the next immediate step?
Q17
A middle aged man complains of upper abdominal pain after a heavy meal. There is tenderness in the upper abdomen and on X-ray, widening of the mediastinum is seen with air in the mediastinum. What is the diagnosis?
Q18
A 20 year old boy is brought to the emergency following a RTA (Road Traffic Accident) with respiratory distress and hypotension. He has subcutaneous emphysema and no air entry on the right side. What is the next best step in the management?
Q19
A man is brought to the emergency after he fell into a man hole and injured his perineum. He feels the urge to micturate but is unable to pass urine and there is blood at the tip of the meatus with extensive swelling of the penis and scrotum. What is the location of the injury?
Q20
Which of the following statements is true regarding retrosternal goiters?