All SubjectsAnatomy (18)Anesthesiology (4)Biochemistry (26)Community Medicine (33)Dental (2)Dermatology (7)ENT (7)Forensic Medicine (13)Internal Medicine (54)Microbiology (21)Obstetrics and Gynecology (28)Ophthalmology (8)Orthopaedics (5)Pathology (25)Pediatrics (18)Pharmacology (27)Physiology (21)Psychiatry (9)Radiology (17)Surgery (23)
Q11
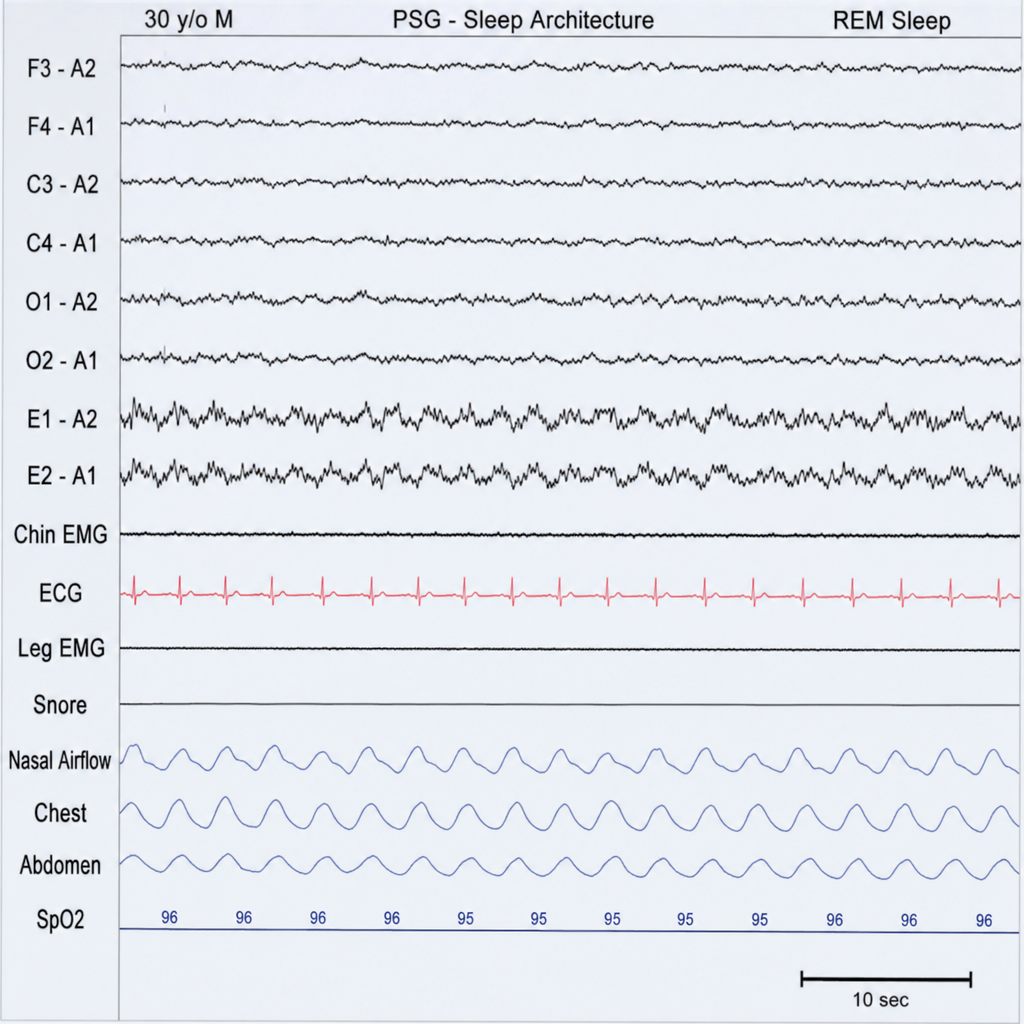
Identify the sleep stage marked in the EEG during the sleep-wake cycle?
Q12
Where does meiosis occur in human females?
Q13
Cerebral blood flow is regulated by all of the following except:
Q14
A patient with pH of 7, pCO2 of 30 mmHg and Bicarbonate levels of 10 meq. What is the acid base abnormality?
Q15
In a preterm baby with respiratory distress syndrome, which type of cell is deficient?
Q16
The lab reports of a patient given below: pH = 7.2, HCO3 = 10 mEq/L, PCO2 = 30 mmHg. This exemplifies which of the following disorders?
Q17
Serum prolactin levels are highest
Q18
Prolactin levels are highest in which of the following?
Q19
In a fetus highest oxygen concentration is found in?
Q20
What does aquaporin deficiency cause?