All SubjectsAnatomy (18)Anesthesiology (4)Biochemistry (26)Community Medicine (33)Dental (2)Dermatology (7)ENT (7)Forensic Medicine (13)Internal Medicine (54)Microbiology (21)Obstetrics and Gynecology (28)Ophthalmology (8)Orthopaedics (5)Pathology (25)Pediatrics (18)Pharmacology (27)Physiology (21)Psychiatry (9)Radiology (17)Surgery (23)
Q11
Patient with pulmonary fibrosis. Which antiarrhythmic drug is contraindicated?
Q12
All-trans retinoic acid is primarily used in the treatment of which of the following tumors?
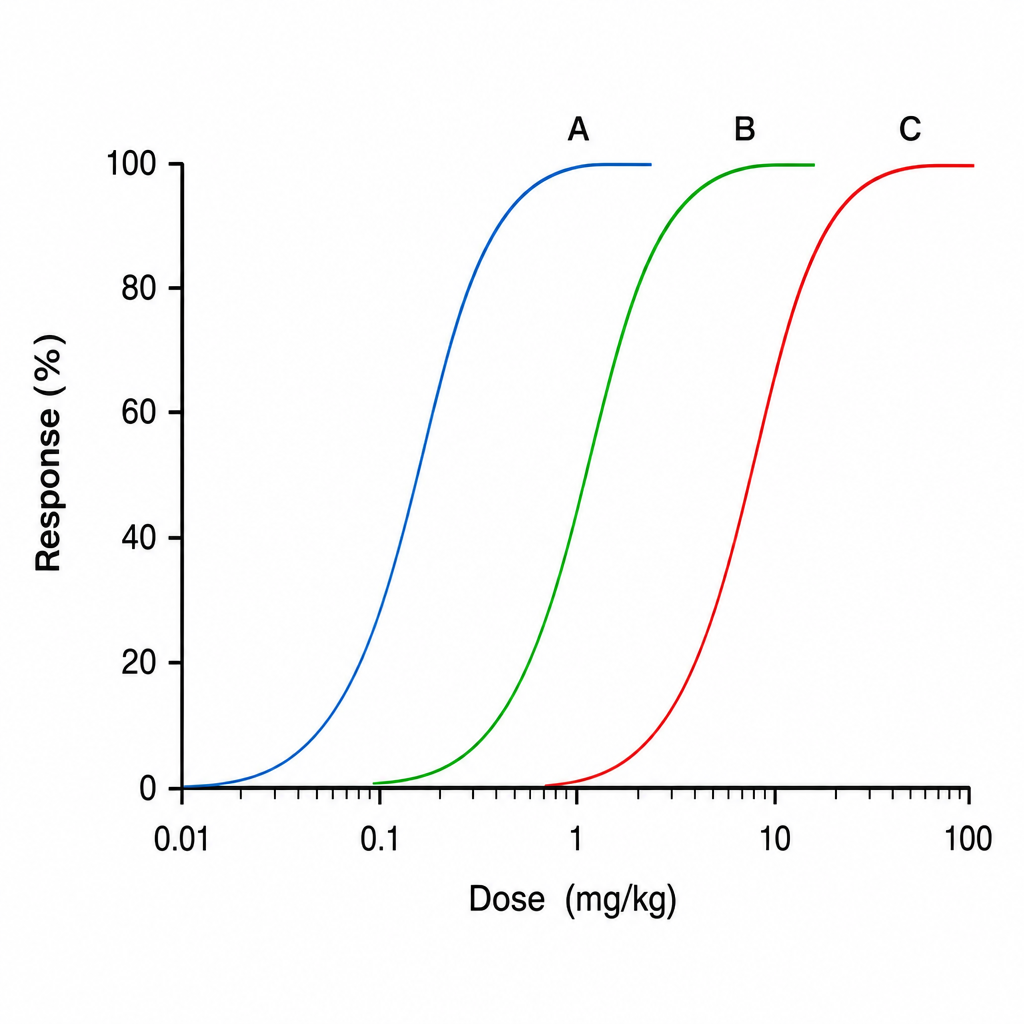
Q13
The graph below shows dose-response curves for three drugs A, B, and C. Which of the following drugs has the highest potency?
Q14
Which of the following antimicrobials should not be given to a chronic asthmatic patient managed on theophylline therapy?
Q15
What is the first-line drug for osteoporosis in postmenopausal women?
Q16
Which drug can be given as a nail lacquer treatment in onychomycosis?
Q17
Drug of choice for post menopausal osteoporosis is
Q18
A patient of biliary colic presented to hospital. Intern gave an injection and the pain worsened. Which is the most likely injection given?
Q19
Which of the following drugs act by inhibiting DNA replication?
Q20
Agent that acts through tyrosine kinase receptor is