All SubjectsAnatomy (18)Anesthesiology (4)Biochemistry (26)Community Medicine (33)Dental (2)Dermatology (7)ENT (7)Forensic Medicine (13)Internal Medicine (54)Microbiology (21)Obstetrics and Gynecology (28)Ophthalmology (8)Orthopaedics (5)Pathology (25)Pediatrics (18)Pharmacology (27)Physiology (21)Psychiatry (9)Radiology (17)Surgery (23)
Q11
Which of the following, if normal, would be most significant in making PEM unlikely?
Q12
A 5-year-old boy has recurrent infections, low platelet count, and rash as shown below. What is the likely diagnosis?

Q13
A 5-year-old unvaccinated child presents to the OPD with fever, red eyes, and a maculopapular rash. What is the most likely complication associated with this condition?
Q14
A 24 month child, with a weight of 11 kg, has RR of 38 / min, chest indrawing, cough and fever. Management according to IMNCI?
Q15
A 5-year-old child is having acute liver failure. Which one of the following criteria is not included in the King's College criteria?
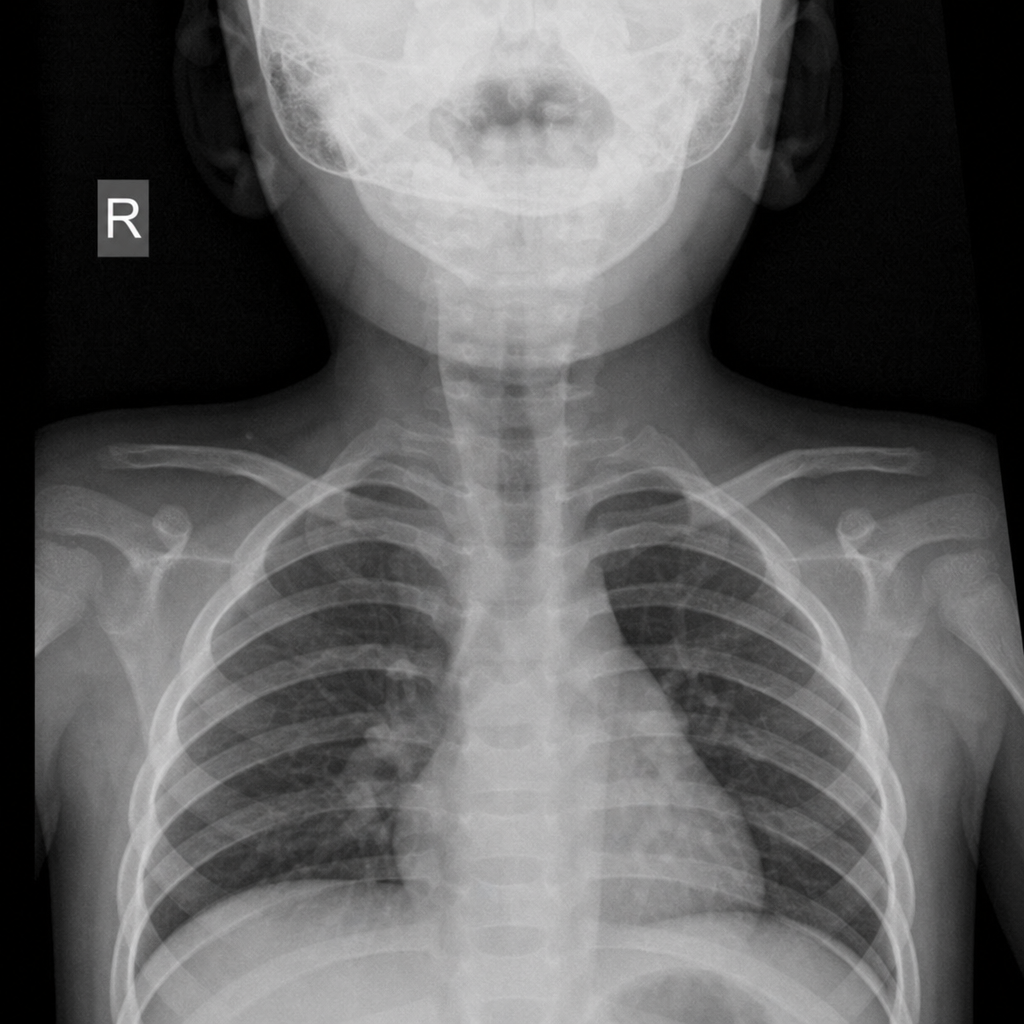
Q16
A 2-year-old child presented with the following x-ray finding. What is the most likely diagnosis?
Q17
Pulmonary plethora in a child presenting with cyanosis, is seen in?
Q18
A boy after playing football complaining fatigue and abdominal pain. He also had a history of hand swelling in past. On ultrasonography, he has shrunken spleen. What is the likely diagnosis of this patient?