NEET-PG 2020 — Pediatrics
16 Previous Year Questions with Answers & Explanations
In a term baby who is 72 hours old, breastfeeding well, and has a bilirubin level of 14 mg/dL, which of the following statements is true?
What is the most serious complication of measles?
Which condition is characterized by conjunctival injection, pharyngeal injection, polymorphic rash, and cervical lymphadenopathy?
Which antibody is not transmitted from mother to baby?
In a preterm baby with respiratory distress syndrome, which type of cell is deficient?
A 4-year-old male child presents with muscle weakness. His mother reports that her child has difficulty in climbing stairs and getting up from the floor. On muscle biopsy, small degenerated muscle fibers and absence of dystrophin were found. What is the diagnosis?
A 2 years old child presents to PHC with fever and cough. He has chest in-drawing and respiratory rate of 38 per minute, weight 11 kg. The next step in management according to IMNCI is:
A term neonate, with a birth weight of 2700 g, who is otherwise well, and is exclusively breastfed, presents for routine evaluation. His total serum bilirubin is found to be 14mg/dl on day 5. What is the management?
A 2 year child presented with low grade fever and stridor. What is the likely diagnosis?
Which of the following, if normal, would be most significant in making PEM unlikely?
NEET-PG 2020 - Pediatrics NEET-PG Practice Questions and MCQs
Question 1: In a term baby who is 72 hours old, breastfeeding well, and has a bilirubin level of 14 mg/dL, which of the following statements is true?
- A. Exchange transfusion
- B. Continue to breastfeed (Correct Answer)
- C. Phototherapy
- D. None of the options
Explanation: ***Continue to breastfeed*** - A bilirubin level of **14 mg/dL at 72 hours of age** in a healthy, full-term, breastfeeding baby is usually within the range considered **physiological jaundice** and does not warrant stopping breastfeeding. - **Breastfeeding should continue** regardless of jaundice management, as interruption can cause a **decrease in milk supply** and may worsen jaundice by reducing bilirubin excretion through stool. - Continued breastfeeding (8-12 times per day) helps promote bilirubin clearance. *Exchange transfusion* - This is an **invasive procedure** reserved for very high bilirubin levels (typically **>20-25 mg/dL** in full-term infants depending on age and risk factors) or in cases of **acute bilirubin encephalopathy**. - A bilirubin level of 14 mg/dL is **well below the threshold** for exchange transfusion in a healthy term infant. *Phototherapy* - According to **AAP guidelines**, phototherapy thresholds are age-dependent: - At **72 hours of age**, phototherapy is typically considered at bilirubin levels **>15-18 mg/dL** in low-risk term infants. - At 14 mg/dL, **close monitoring** with repeat bilirubin measurement is appropriate, but phototherapy is generally **not yet indicated** for a healthy term infant without risk factors. *None of the options* - This option is incorrect because **continuing to breastfeed** is the appropriate and evidence-based management for this clinical scenario. - The other interventions (exchange transfusion, phototherapy) are **not indicated** at this bilirubin level and age in a healthy term infant.
Question 2: What is the most serious complication of measles?
- A. Croup
- B. Otitis media
- C. Meningo-encephalitis
- D. Pneumonia (Correct Answer)
Explanation: ***Pneumonia*** - **Pneumonia**, particularly **giant cell pneumonia**, is the most common cause of **measles-related deaths** in young children. - It results from the **direct viral infection** of the lungs or a **secondary bacterial superinfection**. *Croup* - **Croup (laryngotracheobronchitis)** can be a complication of measles, but it is typically **less severe** and **less life-threatening** than pneumonia. - It primarily affects the **upper airways**, causing a barking cough and stridor. *Meningo-encephalitis* - **Meningo-encephalitis** is a serious, albeit **less common**, complication of measles, occurring in approximately 1 in 1,000 cases. - While potentially fatal or leading to neurological sequelae, it is **outranked by pneumonia** in terms of overall mortality attributed to measles. *Otitis media* - **Otitis media** (middle ear infection) is a common complication of measles, but it is generally **not life-threatening**. - It usually responds well to **antibiotic treatment** and rarely leads to severe outcomes.
Question 3: Which condition is characterized by conjunctival injection, pharyngeal injection, polymorphic rash, and cervical lymphadenopathy?
- A. Kawasaki syndrome (Correct Answer)
- B. Measles
- C. Scarlet fever
- D. Mumps
Explanation: ***Kawasaki syndrome*** - **Kawasaki syndrome** is characterized by a constellation of symptoms including **conjunctival injection**, **pharyngeal injection**, a **polymorphic rash**, and **cervical lymphadenopathy**, often described as the CRASH and burn criteria (Conjunctivitis, Rash, Adenopathy, Strawberry tongue, Hand/foot changes, and Fever). - It is an acute systemic vasculitis, primarily affecting young children, and without treatment, it can lead to **coronary artery aneurysms**. *Measles* - Measles is characterized by a maculopapular rash that typically starts on the face and spreads downwards (cephalocaudal), along with the presence of **Koplik spots** on the buccal mucosa. - While it presents with conjunctivitis and rash, the rash is not polymorphic in the same way as Kawasaki, and cervical lymphadenopathy is less prominent. *Scarlet fever* - **Scarlet fever** is caused by Group A Streptococcus and presents with pharyngitis, fever, and a characteristic **sandpaper-like erythematous rash** with circumoral pallor. - While it has pharyngeal involvement and rash, it lacks the **conjunctival injection** and **polymorphic nature of the rash** seen in Kawasaki syndrome. The rash is typically fine and blanching. - Cervical lymphadenopathy may be present but the overall constellation differs from Kawasaki. *Mumps* - Mumps is an acute viral infection primarily characterized by the swelling of the **parotid glands** (parotitis), often accompanied by fever, headache, and malaise. - It does not typically present with conjunctival injection, a polymorphic rash, or prominent cervical lymphadenopathy as seen in Kawasaki syndrome.
Question 4: Which antibody is not transmitted from mother to baby?
- A. Tetanus IgG antibodies
- B. IgA antibodies (Correct Answer)
- C. Diphtheria IgG antibodies
- D. Measles IgG antibodies
Explanation: ***IgA antibodies*** - While IgA is found in breast milk and provides **passive immunity** to the infant's gastrointestinal tract, it is **not transferred across the placenta** to the fetus. - This antibody has a larger molecular structure and is primarily involved in **mucosal immunity**, making it unsuitable for transplacental transfer. *Diphtheria IgG antibodies* - **IgG antibodies**, including those for diphtheria, are actively transported across the **placenta** from mother to fetus during the third trimester. - This transfer provides the newborn with **passive immunity** against diphtheria during the first few months of life. *Tetanus IgG antibodies* - Similar to diphtheria IgG, **tetanus IgG antibodies** are efficiently transported across the **placenta** from mother to baby. - This offers crucial **passive protection** against tetanus, particularly important after birth. *Measles IgG antibodies* - **Measles IgG antibodies** from a vaccinated or previously infected mother cross the **placenta** to the fetus. - This maternal transfer provides temporary **passive immunity** to the newborn against measles.
Question 5: In a preterm baby with respiratory distress syndrome, which type of cell is deficient?
- A. Type 2 alveolar cell (Correct Answer)
- B. Type 1 alveolar cell
- C. Alveolar capillary endothelial cell
- D. Bronchial mucosal epithelial cell
Explanation: ***Type 2 alveolar cell*** - **Type 2 alveolar cells** (pneumocytes) are responsible for producing and secreting **surfactant**. - A deficiency in these cells, common in preterm infants, leads to insufficient surfactant, causing alveolar collapse and respiratory distress syndrome. *Type 1 alveolar cell* - **Type 1 alveolar cells** are primarily involved in **gas exchange** due to their thin, flat structure. - While essential for respiration, their deficiency is not the primary cause of respiratory distress syndrome in preterm infants. *Alveolar capillary endothelial cell* - **Alveolar capillary endothelial cells** form the walls of the capillaries surrounding the alveoli, facilitating the transfer of gases between the alveoli and blood. - They do not produce surfactant, and their deficiency is not the direct cause of respiratory distress syndrome. *Bronchial mucosal epithelial cell* - **Bronchial mucosal epithelial cells** line the airways and are involved in mucus production and ciliary clearance. - While important for respiratory function, their primary role is not in preventing alveolar collapse in respiratory distress syndrome.
Question 6: A 4-year-old male child presents with muscle weakness. His mother reports that her child has difficulty in climbing stairs and getting up from the floor. On muscle biopsy, small degenerated muscle fibers and absence of dystrophin were found. What is the diagnosis?
- A. Myotonic dystrophy
- B. Becker's muscle dystrophy
- C. Limb-girdle muscular dystrophy
- D. Duchenne muscular dystrophy (Correct Answer)
Explanation: ***Duchenne muscular dystrophy*** - The classic presentation of a young boy with **progressive muscle weakness**, difficulty climbing stairs (**Gowers' sign**), and **absent dystrophin** on muscle biopsy is characteristic of Duchenne muscular dystrophy. - It is an **X-linked recessive disorder** that leads to severe muscle degeneration and weakness due to a complete lack of functional dystrophin protein. *Myotonic dystrophy* - This condition is characterized by **myotonia** (delayed relaxation of muscles after contraction) and typically affects adults, although congenital forms exist. - While it causes muscle weakness, the primary differentiating feature of **myotonia** and its later onset are not present in this case. *Becker's muscle dystrophy* - Becker's muscular dystrophy (BMD) is also an X-linked recessive disorder and a milder form of muscular dystrophy, caused by a **reduced but still functional dystrophin** protein. - Patients with BMD typically present later in childhood or adolescence with slower progression and **some dystrophin** presence, unlike the absent dystrophin and early onset here. *Limb-girdle muscular dystrophy* - This is a group of muscular dystrophies that primarily affect the **pelvic and shoulder girdle muscles**. - It can present with similar weakness, but the **complete absence of dystrophin** found on biopsy points specifically to Duchenne muscular dystrophy, not typical limb-girdle dystrophy, which involves other genetic defects.
Question 7: A 2 years old child presents to PHC with fever and cough. He has chest in-drawing and respiratory rate of 38 per minute, weight 11 kg. The next step in management according to IMNCI is:
- A. Give antibiotics and re-assess in 3 days
- B. Refer to tertiary care
- C. Give antibiotics and refer to tertiary centre (Correct Answer)
- D. Only antipyretics are given
Explanation: ***Give antibiotics and refer to tertiary centre*** - The child presents with **cough**, **fever**, and **chest in-drawing** with a respiratory rate of **38/minute**. According to **IMNCI guidelines**, the presence of **chest in-drawing** in a child aged 2 months to 5 years classifies the condition as **SEVERE PNEUMONIA**. - For severe pneumonia, IMNCI protocol mandates **urgent referral to a hospital** where the child can receive injectable antibiotics (e.g., IV/IM ampicillin or ceftriaxone) and appropriate monitoring. - The child should be given the **first dose of appropriate antibiotic** at the PHC level before referral to prevent deterioration during transport. - This is the correct management approach combining immediate antibiotic therapy with necessary referral for severe disease. *Give antibiotics and re-assess in 3 days* - This management is appropriate for **simple pneumonia** (fast breathing without chest in-drawing), where oral antibiotics can be given at home with reassessment in 2-3 days. - However, in the presence of **chest in-drawing**, the classification escalates to **severe pneumonia**, which requires hospital-level care with injectable antibiotics and monitoring, not outpatient management. - Managing severe pneumonia at PHC without referral risks complications like respiratory failure, sepsis, or death. *Only antipyretics are given* - This is completely inadequate for a child with **severe pneumonia** (chest in-drawing). - Fever management alone does not address the underlying **bacterial infection** requiring antibiotic therapy. - This approach would lead to disease progression and potentially fatal complications. *Refer to tertiary care* - While referral is correct, giving the **first dose of antibiotic before referral** is a critical component of IMNCI protocol. - Pre-referral antibiotic administration helps prevent deterioration during transport and initiates early treatment. - Therefore, "give antibiotics AND refer" is more complete than referral alone.
Question 8: A term neonate, with a birth weight of 2700 g, who is otherwise well, and is exclusively breastfed, presents for routine evaluation. His total serum bilirubin is found to be 14mg/dl on day 5. What is the management?
- A. No active treatment required (Correct Answer)
- B. Stop breastfeeding for 2 days
- C. Phototherapy
- D. Exchange transfusion
Explanation: ***No active treatment required*** - A total serum bilirubin of **14 mg/dL** on day 5 in an otherwise well, exclusively breastfed term neonate (birth weight 2700g, which is >2500g) falls within the **physiologic jaundice range** and below thresholds for intervention. - This level is considered **normal for breastfed infants** at this age and does not warrant medical intervention as per current guidelines. *Stop breastfeeding for 2 days* - This intervention, known as **breast milk jaundice interruption**, is usually reserved for higher bilirubin levels or if there is concern for significant breast milk jaundice, which is not indicated here. - Temporarily stopping breastfeeding can disrupt the establishment of breastfeeding and is generally discouraged unless strictly necessary. *Phototherapy* - **Phototherapy** is indicated for bilirubin levels typically >15-18 mg/dL in a healthy term neonate on day 5, depending on risk factors, which this infant does not meet. - It works by converting unconjugated bilirubin into water-soluble isomers that can be excreted more easily. *Exchange transfusion* - **Exchange transfusion** is reserved for severe hyperbilirubinemia, usually with bilirubin levels approaching or exceeding 20-25 mg/dL, especially if there are signs of **acute bilirubin encephalopathy**. - This level is far below the threshold for such an invasive procedure.
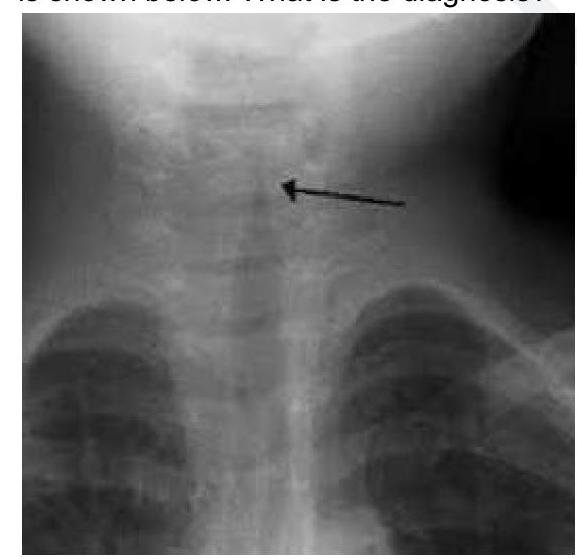
Question 9: A 2 year child presented with low grade fever and stridor. What is the likely diagnosis?
- A. Acute Laryngotracheobronchitis (Correct Answer)
- B. Acute Bacterial Tracheitis
- C. Acute Epiglottitis
- D. Foreign Body aspiration
Explanation: ***Acute Laryngotracheobronchitis*** - The combination of **low-grade fever** and **stridor** in a 2-year-old child strongly suggests **croup**, which is medically known as acute laryngotracheobronchitis. - Croup is characterized by **inflammation** of the larynx, trachea, and bronchi, often presenting with a **barking cough** and inspiratory stridor. The X-ray image would show the characteristic **steeple sign**. *Acute Bacterial Tracheitis* - This is a more severe bacterial infection that can present with stridor but typically shows **higher fever**, **toxic appearance**, and rapid clinical deterioration. - Unlike croup, bacterial tracheitis patients appear **more ill** and may have **purulent secretions** requiring more aggressive management. *Acute Epiglottitis* - A serious condition characterized by **rapid onset of high fever**, **dysphagia**, drooling, and a **"tripod" position**, which are not indicated by the given symptoms. - The stridor in epiglottitis is typically quieter and may indicate more severe airway obstruction compared to the characteristic stridor of croup. *Foreign Body aspiration* - While foreign body aspiration can cause stridor, it is typically an **acute event** with a sudden onset of choking, coughing, and respiratory distress. - There is no mention of a choking episode or sudden onset, and a low-grade fever is less typical for an uncomplicated foreign body aspiration.
Question 10: Which of the following, if normal, would be most significant in making PEM unlikely?
- A. Lean body mass (Correct Answer)
- B. Serum Potassium
- C. Skin fold thickness
- D. Extracellular fluid (ECF)
Explanation: ***Lean body mass*** - A normal **lean body mass** indicates adequate muscle and organ tissue, which is the primary component affected by **Protein-Energy Malnutrition (PEM)**. - Maintaining normal lean body mass despite potential weight loss makes significant PEM, especially the **marasmic type**, less likely. *Extracellular fluid (ECF)* - **Extracellular fluid (ECF)** can be normal or even increased in cases of **edematous PEM** (kwashiorkor) due to decreased oncotic pressure, making it an unreliable indicator for excluding PEM. - Normal ECF does not rule out the depletion of protein, fat, and muscle mass that characterizes PEM. *Serum Potassium* - **Serum potassium** levels can be normal or abnormal (low or high) in PEM depending on hydration status, renal function, and refeeding syndrome, making it a non-specific indicator for excluding the condition. - It does not directly reflect the overall **nutritional status** or body composition changes seen in PEM. *Skin fold thickness* - **Skin fold thickness** measures subcutaneous fat stores, which can be normal or even preserved in some forms of PEM, particularly **kwashiorkor**, even when severe protein deficiency exists. - While reduced skin fold thickness suggests **marasmus**, a normal value does not conclusively rule out **protein deficiency** or other forms of PEM.