All SubjectsAnatomy (18)Anesthesiology (4)Biochemistry (26)Community Medicine (33)Dental (2)Dermatology (7)ENT (7)Forensic Medicine (13)Internal Medicine (54)Microbiology (21)Obstetrics and Gynecology (28)Ophthalmology (8)Orthopaedics (5)Pathology (25)Pediatrics (18)Pharmacology (27)Physiology (21)Psychiatry (9)Radiology (17)Surgery (23)
Q11
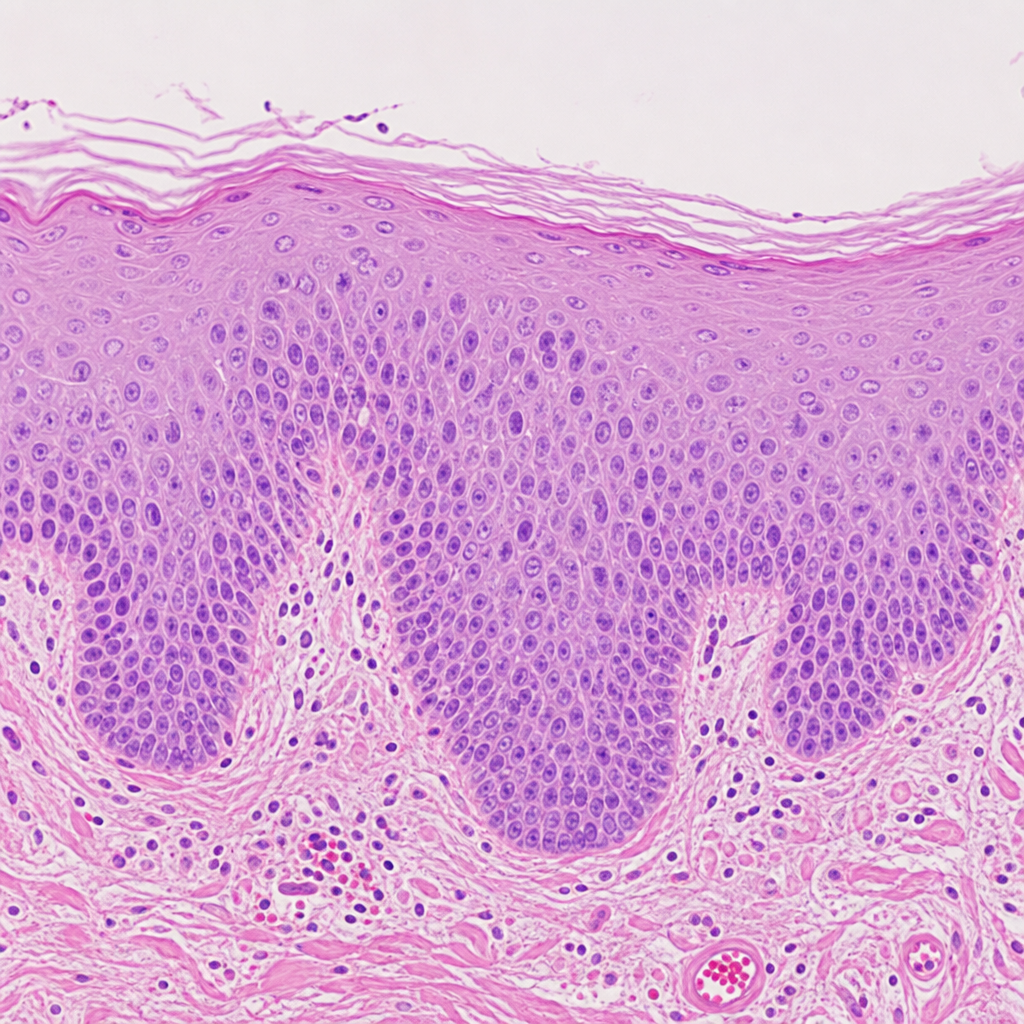
A 45-year-old man who is a chronic smoker came to the clinic with a complaint of cough. The physician examines the patient and takes a biopsy. The biopsy image is provided below. Which of the following cellular changes has happened to this patient?
Q12
In RDS in a child, which cells are found defective?
Q13
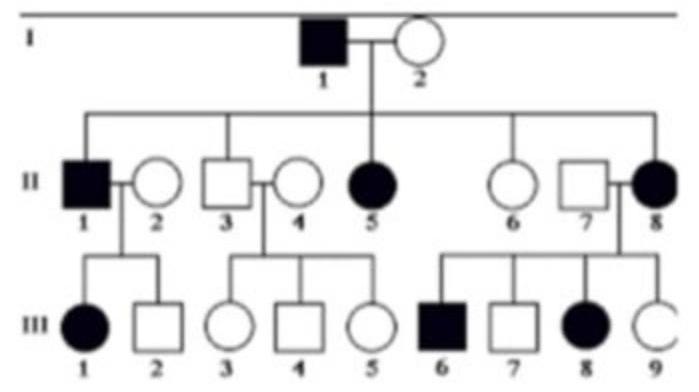
25-year-old man presents for a routine physical examination. The patient is tall and on examination, he was found to have an early diastolic murmur. His family pedigree is given below (image attached). Which of the following is the mode of inheritance by which the disease is likely to be transmitted?
Q14
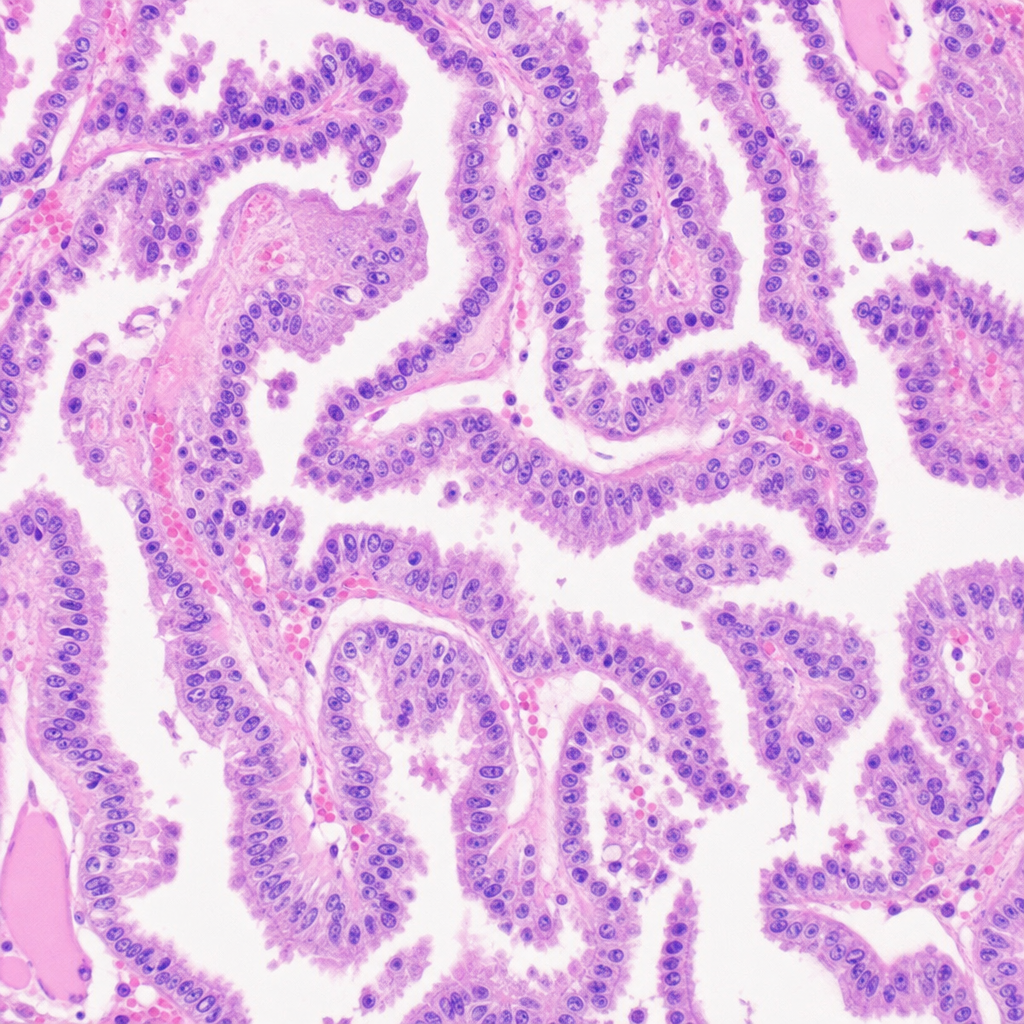
A 25-Year-old male presented with a 2cm thyroid nodule. A thyroidectomy was done. The histology picture is given below. What could be the diagnosis?
Q15
Loss of foot process is classical in case of?
Q16
Which of the following is associated with pauci-immune glomerulonephritis?
Q17
Microscopic examination of the reperfused myocardium is likely to have which of the following findings?
Q18
Loss of foot processes seen on electron microscopy of renal biopsy is a classical feature in which of the following?
Q19
Large, irregular and friable vegetations are seen in?
Q20
Which of the following is a cause of Hirschsprung disease in a patient?