NEET-PG 2020 — Pathology
17 Previous Year Questions with Answers & Explanations
A 30-year-old male presents with swelling around the knee joint. Histopathological examination reveals many giant cells interspersed with mononuclear cells. What is the most likely diagnosis?
A 35-year-old woman with a long history of dyspnea, chronic cough, sputum production, and wheezing dies of respiratory failure following a bout of lobar pneumonia. She was not a smoker or an alcoholic. Which of the following underlying conditions is most likely associated with the pathologic changes shown in the lung autopsy?
HBsAg is based on which principle
Identify the condition shown in the image.

Which of the following factors play a major role in the initiation of thrombus formation?
A 5-year-old child presented with a history of blood in the stools. On examination, there was a polypoid mass in the rectum, a biopsy of which showed as below. The most probable diagnosis is?
A 20-year-old man presented with a complaint of a swelling of the wrist for the last two years. Histopathological examination showed spindle-shaped cells and Verocay bodies. What is the diagnosis?
A 40-year-old person presented with a swelling in the retroperitoneal area. A biopsy from the lesion is as shown below. Molecular analysis demonstrated t(12;16). What is the most probable diagnosis?
A 30-year-old woman presents with thyroid swelling. On investigations, her TSH levels are found to be elevated. Postoperative reports showed lymphocytic infiltration and Hurthle cells. A most probable diagnosis is?
Loss of foot process is classical in case of?
NEET-PG 2020 - Pathology NEET-PG Practice Questions and MCQs
Question 1: A 30-year-old male presents with swelling around the knee joint. Histopathological examination reveals many giant cells interspersed with mononuclear cells. What is the most likely diagnosis?
- A. Osteosarcoma
- B. Ewing's sarcoma
- C. Giant cell tumour (Correct Answer)
- D. Chondrosarcoma
Explanation: ***Giant cell tumour*** - The presence of **giant cells** interspersed with **mononuclear cells** in the histopathological examination is characteristic of giant cell tumors [1], often found around the **knee joint** [1]. - Typically occurs in **young adults** and is associated with **subarticular bone lesions** that cause joint swelling [1]. *Osteosarcoma* - Generally presents with **extensive bone destruction** and **persistent pain**, along with a mass, not primarily giant cell formation. - Commonly involves individuals aged **10-20 years**, making it less likely in a 30-year-old male. *Ewing's sarcoma* - Characterized by **small round blue cells** on histology, often with **more aggressive behavior** and less prominent giant cells. - Typically affects the **pelvis** and **long bones**, rather than directly around the knee joint. *Chondrosarcoma* - Primarily characterized by **cartilage formation** with no prominent giant cells, often leading to a confusing diagnosis in imaging. - Usually occurs in **older adults** and does not typically present with predominant giant cells in histopathology. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Bones, Joints, and Soft Tissue Tumors, pp. 1205-1206.
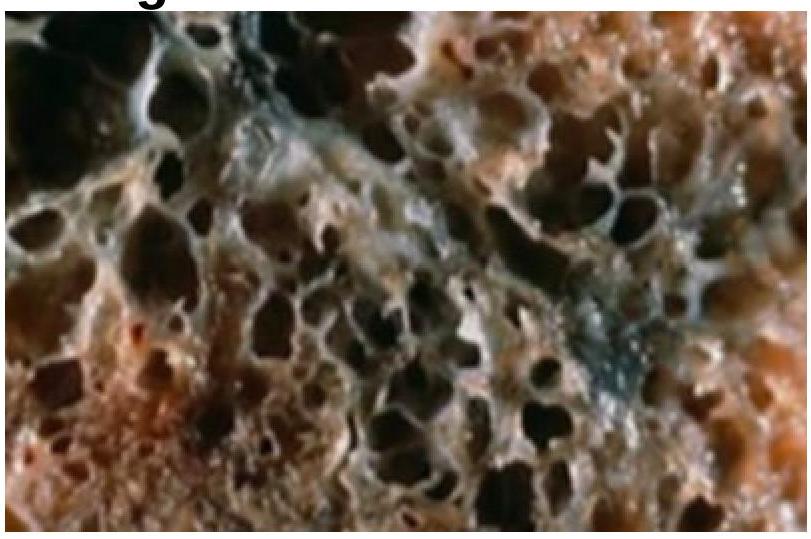
Question 2: A 35-year-old woman with a long history of dyspnea, chronic cough, sputum production, and wheezing dies of respiratory failure following a bout of lobar pneumonia. She was not a smoker or an alcoholic. Which of the following underlying conditions is most likely associated with the pathologic changes shown in the lung autopsy?
- A. Antibodies against type 4 collagen (associated with Goodpasture syndrome)
- B. Cystic fibrosis (a genetic disorder affecting the lungs)
- C. Mutation in dynein arms (associated with primary ciliary dyskinesia)
- D. Alpha-1 antitrypsin deficiency (Correct Answer)
Explanation: ***Alpha 1 antitrypsin deficiency*** - This condition leads to **accumulation of abnormal protein** in the liver and lungs, resulting in emphysema, which is consistent with chronic cough and dyspnea [1]. - Patients often develop **lung pathology** similar to what is seen in smokers, making it plausible given the patient's background [1]. *Mutation in dynein arms* - This is associated with **primary ciliary dyskinesia**, which presents with recurrent respiratory infections but is not typical in non-smokers or in the context of **dyspnea with chronic cough**. - Usually linked to **situs inversus** and **recurrent infections**, neither of which is highlighted here. *Antibodies against type 4 collagen* - This condition is related to **Goodpasture syndrome**, which typically results in **hemoptysis** and **renal failure**, rather than chronic cough and sputum production. - The predominant involvement in this syndrome does not align with the clinical presentation of **chronic lung disease** noted in this patient. *Cystic fibrosis* - While it causes **chronic respiratory symptoms**, it is usually seen in younger patients and is associated with **pancreatic insufficiency** and **salty sweat**. - The age of the patient and symptom progression does not fit well with a diagnosis of cystic fibrosis. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Lung, pp. 683-684.
Question 3: HBsAg is based on which principle
- A. Chemiluminescence
- B. Immunofluorescence
- C. Immunochromatography assays
- D. ELISA (Correct Answer)
Explanation: ***ELISA*** - **Enzyme-linked immunosorbent assay (ELISA)** is a widely used laboratory test to detect and quantify antigens (like HBsAg) or antibodies in a sample. - It involves an enzyme-linked antibody that reacts with a substrate to produce a detectable signal, making it highly sensitive and specific for **HBsAg detection**. *Immunochromatography assays* - These are typically **rapid diagnostic tests (RDTs)** that provide quick qualitative results, often used for point-of-care testing. - While they can detect HBsAg, they generally have lower sensitivity and specificity compared to ELISA. *Chemiluminescence* - This is a detection method used in some immunoassays where a chemical reaction emits light, often providing higher sensitivity than colorimetric detection. - While it can be incorporated into HBsAg testing platforms, it is a *detection principle* rather than the primary assay principle like ELISA itself. *Immunofluorescence* - This technique uses **fluorescently labeled antibodies** to visualize antigens in cells or tissues under a fluorescence microscope [1]. - It is used for localization and identification of antigens, but not typically the primary method for routine quantitative HBsAg serology [1]. **References:** [1] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. (Basic Pathology) introduces the student to key general principles of pathology, both as a medical science and as a clinical activity with a vital role in patient care. Part 2 (Disease Mechanisms) provides fundamental knowledge about the cellular and molecular processes involved in diseases, providing the rationale for their treatment. Part 3 (Systematic Pathology) deals in detail with specific diseases, with emphasis on the clinically important aspects., pp. 259-260.
Question 4: Identify the condition shown in the image.
- A. Villous adenoma
- B. Hyperplastic polyp
- C. Juvenile polyp
- D. Peutz-Jeghers syndrome (Correct Answer)
Explanation: ***Juvenile polyp*** - Juvenile polyps are commonly found in children and present as **solitary lesions**, usually in the rectum [1]. - They typically appear **smooth**, with a characteristic lobulated surface, emphasizing their benign nature. *Villous adenoma* - Villous adenomas are characterized by **frond-like projections** and have a higher risk of malignant transformation [2]. - These lesions usually occur in adults and are typically larger and more **invasive** compared to juvenile polyps [2]. *Hyperplastic polyp* - Hyperplastic polyps are small, **benign lesions** that result from epithelial overgrowth with a typical **smooth surface** [3]. - They are usually found in the colon and do not present with the distinctive features of juvenile polyps. *Peutz-Jeghers polyp* - Peutz-Jeghers polyps are associated with **Peutz-Jeghers syndrome** and exhibit a **hamartomatous** appearance, often protruding from various gastrointestinal sites [1]. - These polyps are typically more **complex** and can be found in older children and adults, differing significantly from juvenile polyps [1]. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Gastrointestinal Tract, p. 813. [2] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Alimentary System Disease, pp. 371-372. [3] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Gastrointestinal Tract, pp. 811-813.
Question 5: Which of the following factors play a major role in the initiation of thrombus formation?
- A. Vasoconstriction
- B. Coagulation cascade activation
- C. Platelets activation
- D. Endothelial injury (Correct Answer)
Explanation: ***Endothelial injury*** - **Endothelial injury** is a critical initiating factor in thrombus formation, leading to platelet adhesion and activation [1]. - Damage to the endothelium exposes the underlying **collagen** and **tissue factor**, which promote hemostasis and coagulation [2,3,5]. *Vasoconstriction* - While vasoconstriction can reduce blood flow and helps in minimizing blood loss, it is not a direct initiator of thrombus formation. - It primarily acts as a response to injury rather than a trigger for the **clotting mechanism**. *Coagulation cascade activation* - Activation of the coagulation cascade occurs after endothelial injury and is part of the clotting process, not the initiation [2]. - It involves various factors like fibrinogen and prothrombin but is secondary to the initial endothelial damage. *Platelets activation* - Platelet activation is a response to the exposed collagen due to endothelial injury and is not the initial trigger of thrombus formation [3,4,5]. - It occurs as a subsequent step once the endothelial injury has taken place, facilitating plug formation [4]. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Hemodynamic Disorders, Thromboembolic Disease, and Shock, pp. 132-133. [2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Hemodynamic Disorders, Thromboembolic Disease, and Shock, pp. 126-128. [3] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. (Basic Pathology) introduces the student to key general principles of pathology, both as a medical science and as a clinical activity with a vital role in patient care. Part 2 (Disease Mechanisms) provides fundamental knowledge about the cellular and molecular processes involved in diseases, providing the rationale for their treatment. Part 3 (Systematic Pathology) deals in detail with specific diseases, with emphasis on the clinically important aspects., pp. 142-143. [4] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Blood And Bone Marrow Disease, pp. 581-582. [5] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Hemodynamic Disorders, Thromboembolic Disease, and Shock, p. 128.
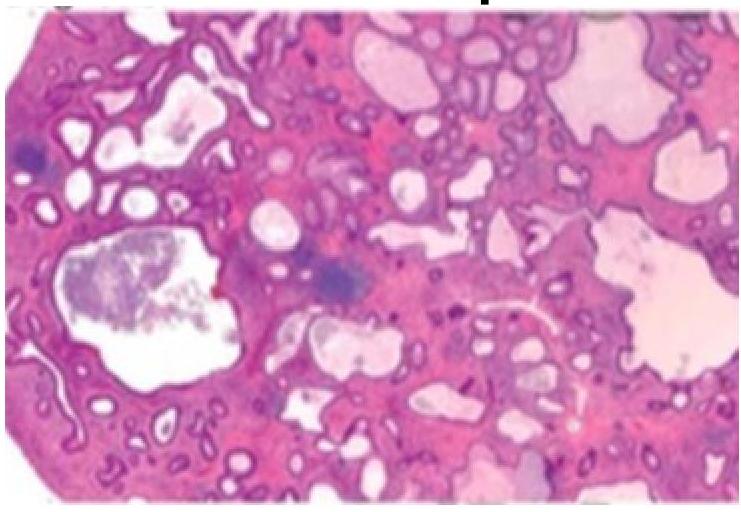
Question 6: A 5-year-old child presented with a history of blood in the stools. On examination, there was a polypoid mass in the rectum, a biopsy of which showed as below. The most probable diagnosis is?
- A. Villous adenoma
- B. Juvenile polyp (Correct Answer)
- C. Vascular malformation
- D. Serrated adenoma
Explanation: ***Juvenile polyp*** - The image shows **dilated, cystically appearing glands** within an inflamed lamina propria, which is characteristic of a juvenile polyp. - Juvenile polyps are the most common cause of **rectal bleeding** in children under 10 years of age and are typically benign. *Villous adenoma* - Villous adenomas are **neoplastic polyps** with a **villous (finger-like) architecture** and are more commonly seen in older adults [1]. - They typically show **dysplastic changes** and are considered premalignant [1]. *Vascular malformation* - Vascular malformations consist of **abnormally formed blood vessels** (e.g., arteriovenous malformations, hemangiomas) and would appear as dilated or aberrant vessels on histology. - While they can cause bleeding, the image does not show a predominance of vascular structures. *Serrated adenoma* - Serrated adenomas are characterized by **sawtooth-like glandular infoldings** and show varying degrees of dysplasia. - They are typically found in adults and are considered premalignant, not benign growths usually found in children. **References:** [1] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Alimentary System Disease, pp. 371-372.
Question 7: A 20-year-old man presented with a complaint of a swelling of the wrist for the last two years. Histopathological examination showed spindle-shaped cells and Verocay bodies. What is the diagnosis?
- A. Lipoma
- B. Dermoid cyst
- C. Neurofibroma
- D. Schwannoma (Correct Answer)
Explanation: ***Schwannoma*** - Characterized by the presence of **spindle-shaped cells** and **Verocay bodies**, typical of schwannomas, which are tumors of peripheral nerve sheath origin [1,3]. - Commonly presents with **pain** and **local swelling** in affected areas, aligning with the patient's symptoms [2]. *Dermoid cyst* - Usually presents as a **cystic lesion** containing skin appendages but does not feature spindle-shaped cells. - Lacks the characteristic **Verocay bodies**, which help differentiate schwannomas [1]. *Lipoma* - Composed of **mature adipocytes**, presenting as soft, movable masses, but not associated with spindle-shaped cells. - Histopathological examination would not reveal **Verocay bodies**, making it distinct from schwannoma [1]. *Neurofibroma* - Typically associated with **plexiform growth patterns** and lacks the classic **Verocay bodies** seen in schwannomas [1]. - Often occurs in patients with **neurofibromatosis** and presents differently than the clinical scenario here [3]. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Peripheral Nerves and Skeletal Muscles, p. 1250. [2] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Manifestations Of Central And Peripheral Nervous System Disease, pp. 727-728. [3] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Peripheral Nerves and Skeletal Muscles, pp. 1248-1249.
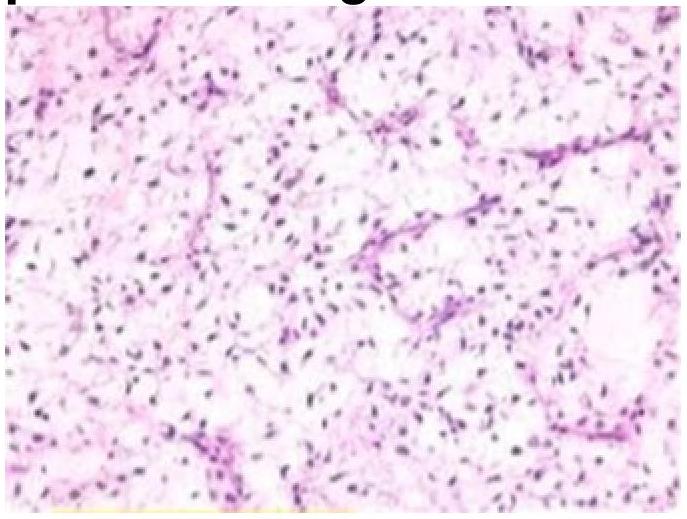
Question 8: A 40-year-old person presented with a swelling in the retroperitoneal area. A biopsy from the lesion is as shown below. Molecular analysis demonstrated t(12;16). What is the most probable diagnosis?
- A. Myxoid liposarcoma (Correct Answer)
- B. Benign lipoma
- C. Synovial sarcoma
- D. Pleomorphic sarcoma
Explanation: ***Myxoid liposarcoma*** - The presence of **t(12;16)** translocation is characteristic of myxoid liposarcoma, which is crucial for diagnosis [1]. - Typically presents as a **soft tissue mass**, often in the retroperitoneum, consistent with the patient's swelling [1]. *Pleomorphic sarcoma* - Does not specifically associate with **t(12;16)** translocation; it is more commonly associated with various genetic alterations [1]. - Typically presents as a **heterogeneous** and highly aggressive neoplasm, lacking the specific features noted in this case. *Synovial sarcoma* - More commonly associated with a **t(X;18)** translocation, not t(12;16), which rules it out in this context. - Usually presents around the **joints** and has a different histological pattern compared to liposarcoma. *Lipoma* - A benign tumor that typically does not involve significant genetic mutations like **t(12;16)** [1]. - Presents as a **soft, mobile mass** and does not generally occur in a retroperitoneal setting with this size [1]. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Bones, Joints, and Soft Tissue Tumors, pp. 1222-1223.
Question 9: A 30-year-old woman presents with thyroid swelling. On investigations, her TSH levels are found to be elevated. Postoperative reports showed lymphocytic infiltration and Hurthle cells. A most probable diagnosis is?
- A. Hashimoto's thyroiditis (Correct Answer)
- B. Graves' disease
- C. Follicular thyroid carcinoma
- D. Medullary thyroid carcinoma
Explanation: ***Hashimoto's thyroiditis*** - The presence of **lymphocytic infiltration** and **Hurthle cells** on postoperative pathology is characteristic of Hashimoto's thyroiditis [1,2]. - Elevated **TSH levels** indicate hypothyroidism, which aligns with the autoimmune nature of Hashimoto's affecting thyroid hormone production [1]. *Graves disease* - Typically presents with **hyperthyroidism**, leading to suppressed TSH levels rather than elevation. - Characterized by **thyroid enlargement** and the presence of **autoantibodies** like TSI, not lymphocytic infiltration. *Follicular carcinoma* - While it can cause **thyroid swelling**, it is usually associated with **malignant characteristics** rather than Hurthle cells and lymphocytic infiltration. - TSH levels can be normal, as it does not principally engage in autoimmune thyroid destruction like Hashimoto's. *Medullary carcinoma thyroid* - Originates from **C cells** producing calcitonin, and typically presents with elevated calcitonin levels, not TSH. - Characteristic findings include **C-cell hyperplasia** or **neoplastic changes**, which do not match the presented lymphocytic infiltration. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Endocrine System, pp. 1090-1092. [2] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Liver And Biliary System Disease, pp. 427-428.
Question 10: Loss of foot process is classical in case of?
- A. Segmental glomerulosclerosis (Correct Answer)
- B. Diabetic nephropathy (later stages)
- C. Membranous nephropathy
- D. IgA vasculitis
Explanation: ***Segmental glomerulosclerosis*** - Characterized by a **loss of foot processes**, leading to a "focal" or "segmental" pattern of sclerosis on histology [1][2]. - Often presents with **nephrotic syndrome**, including proteinuria and edema, due to damage to the glomeruli [1][3]. *Membranous glomerulitis* - Primarily involves **thickening of the glomerular capillary walls** without the loss of foot processes initially. - It is often associated with **membrane antibodies** and can lead to nephrotic syndrome, but not specifically linked to foot process loss [2]. *Diabetic nephropathy* - Characterized by **nodular glomerulosclerosis** and other microvascular changes, but the loss of foot processes is not a classic feature. - Typically presents with **diffuse glomerular basement membrane thickening** and eventual renal failure. *IgA nephropathy* - Characterized by the deposition of **IgA antibodies** in the mesangial area, leading to hematuria but not directly causing loss of foot processes. - Symptoms often include **recurrent episodes of hematuria** which can be triggered by infection, rather than nephrotic syndrome. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Kidney, pp. 927-928. [2] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Diseases Of The Urinary And Male Genital Tracts, pp. 530-532. [3] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Kidney, p. 913.