All (366)Anatomy (18)Anesthesiology (4)Biochemistry (26)Community Medicine (33)Dental (2)Dermatology (7)ENT (7)Forensic Medicine (13)Internal Medicine (54)Microbiology (21)Obstetrics and Gynecology (28)Ophthalmology (8)Orthopaedics (5)Pathology (25)Pediatrics (18)Pharmacology (27)Physiology (21)Psychiatry (9)Radiology (17)Surgery (23)
Q301
Episiotomy incision was extended posteriorly beyond perineal body injuring the structure immediately posterior to it. Which structure has been injured?
Q302
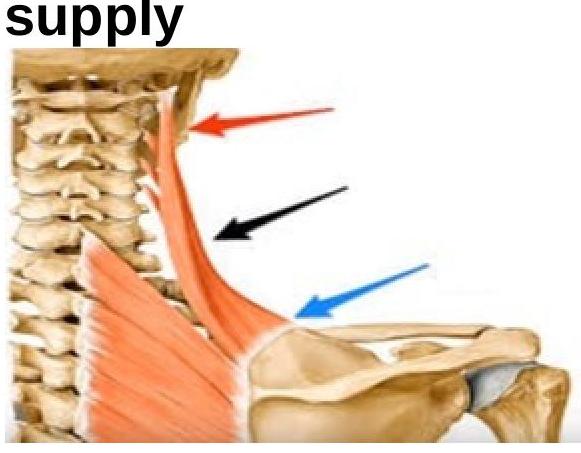
What is the nerve supply of the shown muscle?