All (366)Anatomy (18)Anesthesiology (4)Biochemistry (26)Community Medicine (33)Dental (2)Dermatology (7)ENT (7)Forensic Medicine (13)Internal Medicine (54)Microbiology (21)Obstetrics and Gynecology (28)Ophthalmology (8)Orthopaedics (5)Pathology (25)Pediatrics (18)Pharmacology (27)Physiology (21)Psychiatry (9)Radiology (17)Surgery (23)
Q141
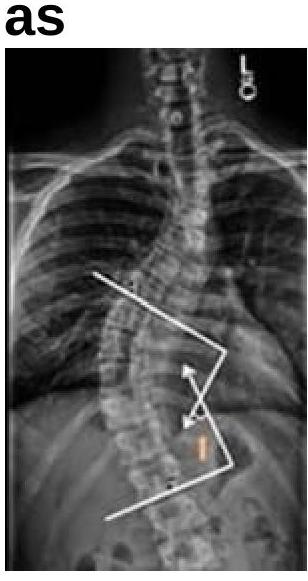
What is the angle shown in the image known as?