All SubjectsAnatomy (18)Anesthesiology (4)Biochemistry (26)Community Medicine (33)Dental (2)Dermatology (7)ENT (7)Forensic Medicine (13)Internal Medicine (54)Microbiology (21)Obstetrics and Gynecology (28)Ophthalmology (8)Orthopaedics (5)Pathology (25)Pediatrics (18)Pharmacology (27)Physiology (21)Psychiatry (9)Radiology (17)Surgery (23)
Q11
Which of the following is not used for postcoital contraception?
Q12
A 7 weeks pregnant lady has 1 accidental exposure to x-ray. Which of the following should be done?
Q13
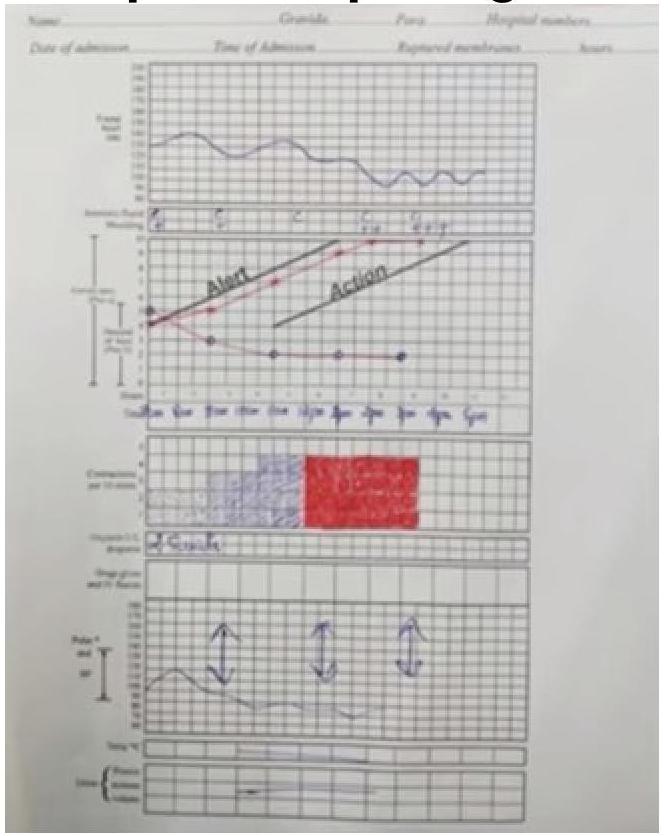
Given the following partogram data, identify the most likely diagnosis: Cervical dilation curve shows a prolonged labor with the cervical dilation falling to the right of the alert line.
Q14
Which of the following is not considered an absolute contraindication for the use of an Intra Uterine Contraceptive Device (IUD)?
Q15
A mother brought her 16-year-old daughter to Gynaecology OPD with a complaint of not attaining menarche. She gives a history of cyclic abdominal pain. On further examination, a midline abdominal swelling is seen. Per rectal examination reveals a bulging mass in the vagina. Which of the following conditions is most likely responsible for these findings?
Q16
A 24-year-old woman who had a home delivery 2 weeks ago now presents with a complete perineal tear. What is the next line of management?
Q17
A woman with 18 weeks gestation presented to the OPD. On abdominal examination, the uterine size was 16 weeks. On USG, oligohydramnios was found, which of the following is suspected?
Q18
35 yr old primigravida conceived after IVF cycle attends obstetrics clinic with 38 weeks gestation. Her obstetric details reveal DiCho-DiAmn twins with 1st twin as breech. Her BP was 140/90 mmHg on 2 occasions with proteinuria +1. How will you manage this case?
Q19
35 yr old lady attends gynaec OPD with excessive bleeding since 6 months, not controlled with non hormonal drugs. USG and clinical examination reveals no abnormality. Next step is?
Q20
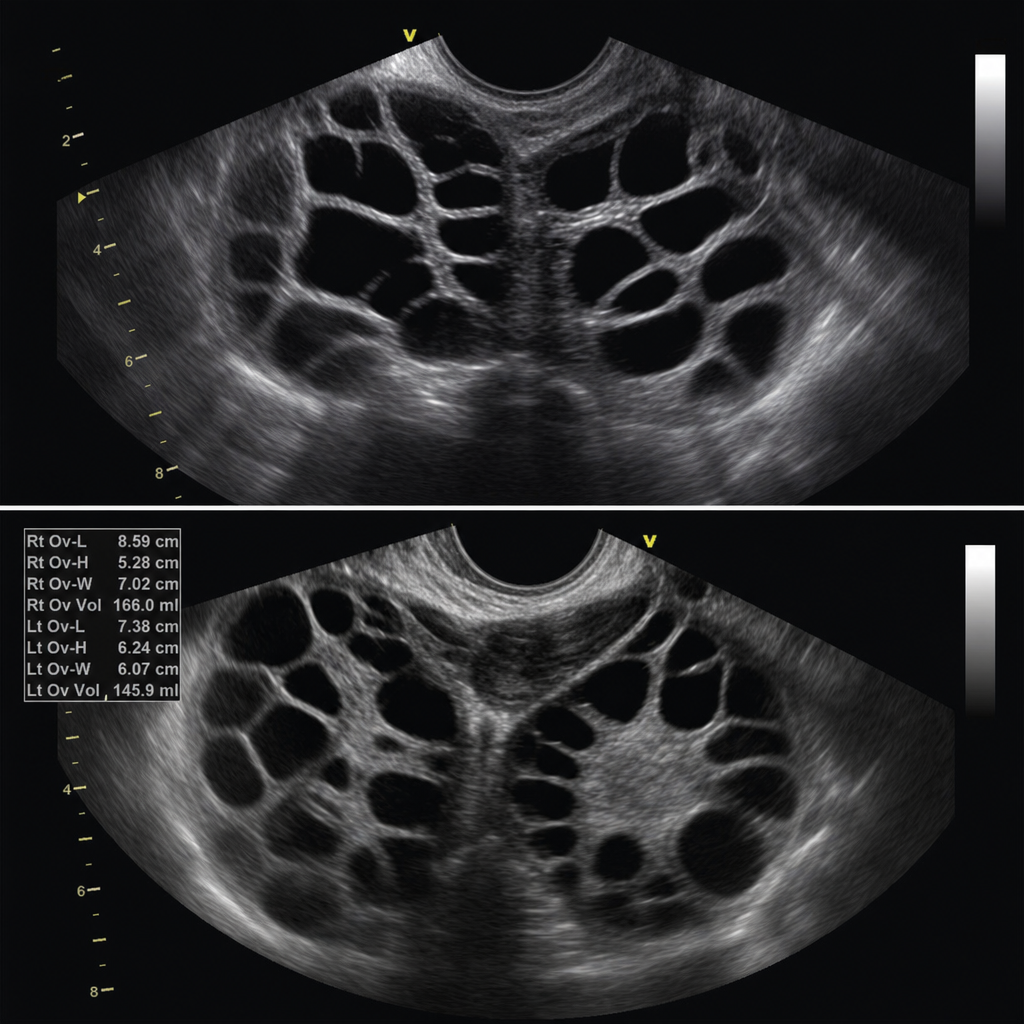
A female undergoing treatment for infertility with IVF was given Inj. HCG, presented with a history of vomiting, nausea, and headache. The USG is shown as below, what is the diagnosis?