Which is the most common pancreatic endocrine neoplasm?
The differentiating feature between IBS and organic GI disease is:
A 51-year-old person came with a complaint of hematuria. On examination, he was normotensive and had pedal edema. Investigations revealed the patient had no glucosuria and had a creatinine value of 9mg%. Renal biopsy is as shown below. Which of the following investigations should be done to identify the etiology of the disease?
A female patient has been on lithium for bipolar disorder for 6 months. After fasting for several days due to religious reasons, she presents with seizures, tremors, confusion, and weakness. What is the most appropriate investigation to diagnose her condition?
The patient presents with unilateral proptosis and bilateral abducent nerve palsy. What is the most likely cause?
Incongruous Homonymous hemianopia with Wernicke's hemianopia pupil is seen with the lesion of
25-year-old man presents for a routine physical examination. The patient is tall and on examination, he was found to have an early diastolic murmur. His family pedigree is given below (image attached). Which of the following is the mode of inheritance by which the disease is likely to be transmitted?
Renal tubular acidosis with ABG value pH = 7.24 PO2=80; PaCO2= 36 Na = 131; HCO3 = 14 Cl= 90; BE = -13 Glucose = 135 the above ABG picture suggests –
What is the Child-Pugh class for a patient who has a serum bilirubin of 2.5 mg/dL, serum albumin of 3 g/dL, INR of 2, mild ascites, but no encephalopathy?
Which of the following is associated with pauci-immune glomerulonephritis?
NEET-PG 2020 - Internal Medicine NEET-PG Practice Questions and MCQs
Question 21: Which is the most common pancreatic endocrine neoplasm?
- A. Insulinoma (Correct Answer)
- B. Gastrinoma
- C. VIPoma
- D. Glucagonoma
Explanation: ***Insulinoma*** - It is the **most common pancreatic endocrine neoplasm**, characterized by excessive insulin production leading to hypoglycemia. - Most patients present with **symptoms of hypoglycemia**, such as sweating, confusion, and palpitations due to overproduction of insulin [1]. *Gastrinoma* - Generally implicated in **Zollinger-Ellison syndrome**, it causes excessive gastric acid secretion, leading to severe ulcers but is less common than insulinoma. - Associated with **diarrhea and abdominal pain**, not typically causing hypoglycemia [1]. *Glucagonoma* - Rarely seen, it causes **hyperglycemia** and characteristic **necrotizing migratory erythema**, rather than hypoglycemic episodes. - Comprises a minority of pancreatic endocrine tumors and is not the most common type. *VIPoma* - Produces **vasoactive intestinal peptide**, leading to profuse watery diarrhea and severe electrolyte imbalance. - It is uncommon compared to insulinoma and primarily causes gastrointestinal symptoms rather than hypoglycemia.
Question 22: The differentiating feature between IBS and organic GI disease is:
- A. Pain abdomen
- B. Mucus in stools
- C. Diarrhea
- D. Presence of inflammation indicated by elevated stool calprotectin (Correct Answer)
Explanation: ***Presence of inflammation indicated by elevated stool calprotectin*** - Elevated **stool calprotectin** is a reliable biomarker for **gastrointestinal inflammation**, indicating an **organic GI disease** such as inflammatory bowel disease (IBD). - **Irritable bowel syndrome (IBS)** is a functional disorder and typically does not involve **inflammation**, so stool calprotectin levels would be normal. *Diarrhea* - **Diarrhea** can be a symptom of both **IBS** (specifically IBS-D) and various **organic GI diseases** (e.g., Crohn's disease, ulcerative colitis, celiac disease) [1]. - Therefore, its presence alone does not differentiate between a functional and an organic cause [1]. *Pain abdomen* - **Abdominal pain** is a cardinal symptom of **IBS**, specifically related to bowel movements [1]. - It is also a very common symptom in many **organic GI diseases**, making it a non-specific differentiating feature. *Mucus in stools* - **Mucus in stools** can occur in **IBS**, often due to increased colonic transit or irritation, but without underlying inflammation [1]. - It can also be present in **organic GI diseases**, particularly those involving inflammation or structural changes in the bowel.
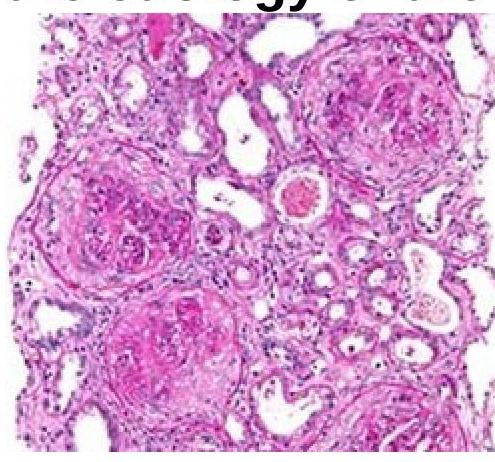
Question 23: A 51-year-old person came with a complaint of hematuria. On examination, he was normotensive and had pedal edema. Investigations revealed the patient had no glucosuria and had a creatinine value of 9mg%. Renal biopsy is as shown below. Which of the following investigations should be done to identify the etiology of the disease?
- A. ANA
- B. ANTI GBM antibodies (Correct Answer)
- C. HIV RNA
- D. Urine immunoelectrophoresis
Explanation: ***ANTI GBM antibodies*** - The presence of hematuria and renal failure suggests a possible **glomerulonephritis**, where **anti-GBM (Glomerular Basement Membrane) antibodies** would help confirm conditions like Goodpasture syndrome [2]. - This test specifically identifies **anti-GBM disease** [1,2], which is crucial in guiding management for this patient with suspected renal pathology [3]. *ANA* - **Antinuclear antibody (ANA)** testing is typically used for autoimmune diseases like **Systemic Lupus Erythematosus** but is less specific for glomerular diseases. - In this context, ANA would not specifically help in identifying the **etiology of renal failure** associated with hematuria. *Urine immunoelectrophoresis* - This test is primarily useful for detecting **light chains** in conditions like **multiple myeloma** and may not be relevant to general hematuria or renal failure. - It is not a direct test for **glomerular disease etiology** related to hematuria and edema. *HIV RNA* - While **HIV** can lead to renal complications, including **HIV-associated nephropathy**, this test is not the first line for etiological determination in this specific presentation. - Negative **HIV serology** doesn't rule out renal disease caused by other factors, making this test less relevant here. **References:** [1] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Diseases Of The Urinary And Male Genital Tracts, pp. 526-527. [2] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Diseases Of The Urinary And Male Genital Tracts, pp. 537-538. [3] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Kidney, pp. 918-919.
Question 24: A female patient has been on lithium for bipolar disorder for 6 months. After fasting for several days due to religious reasons, she presents with seizures, tremors, confusion, and weakness. What is the most appropriate investigation to diagnose her condition?
- A. Serum electrolytes
- B. Serum lithium levels (Correct Answer)
- C. ECG
- D. MRI
Explanation: **Serum lithium levels** - The patient's symptoms (seizures, tremors, confusion, weakness) are classic for **lithium toxicity**. - **Fasting** can lead to dehydration and electrolyte imbalance, which can increase lithium concentrations and toxicity [1]. *Serum electrolytes* - While **electrolyte imbalances** can occur with fasting and contribute to symptoms, measuring serum electrolytes alone will not directly diagnose lithium toxicity. - Electrolyte disturbances might be a predisposing factor or a concomitant issue, but not the primary diagnostic test for lithium toxicity itself [1]. *ECG* - An **ECG** can reveal cardiac effects of lithium toxicity, such as T-wave flattening or inversion, but it is not the most appropriate direct diagnostic test for the condition itself. - ECG changes are secondary manifestations and may not always be present or specific. *MRI* - While an **MRI** of the brain might be considered to rule out other causes of neurological symptoms like a stroke or brain lesion, it is not the initial or most appropriate investigation for suspected lithium toxicity. - The clinical picture strongly points to a pharmacological cause, making laboratory tests more relevant first-line diagnostics than imaging.
Question 25: The patient presents with unilateral proptosis and bilateral abducent nerve palsy. What is the most likely cause?
- A. Cavernous sinus pathology (Correct Answer)
- B. Orbital cellulitis
- C. Orbital pseudotumor
- D. Orbital lymphoma
Explanation: The patient presents with unilateral proptosis and bilateral abducent nerve palsy. What is the most likely cause? ***Cavernous sinus pathology*** - **Unilateral proptosis** combined with **bilateral abducens nerve palsy** is a classic presentation consistent with cavernous sinus involvement, as the abducens nerves (CN VI) pass through both cavernous sinuses and are vulnerable to pathology there. [1] - The cavernous sinus contains multiple cranial nerves (**III, IV, V1, V2, VI**) and the internal carotid artery, making it a critical anatomical location where lesions can cause complex neurological deficits affecting orbital structures and eye movements. [1] *Orbital cellulitis* - Typically presents with **unilateral proptosis**, pain, eyelid swelling, and fever, often following a sinus infection. - It primarily affects the **orbital contents anterior to the orbital septum** and would not explain bilateral abducens nerve palsy. *Orbital pseudotumor* - Characterized by **unilateral proptosis**, pain, and diplopia due to idiopathic inflammation of orbital tissues. - While it can cause ophthalmoplegia, **bilateral abducens nerve palsy** is not a typical presentation for a condition usually confined to one orbit. *Orbital lymphoma* - Presents with **painless, slowly progressive unilateral proptosis** or an orbital mass. - While it can cause compressive symptoms, **bilateral abducens nerve palsy** is an atypical presentation as the disease usually remains confined to a single orbit.
Question 26: Incongruous Homonymous hemianopia with Wernicke's hemianopia pupil is seen with the lesion of
- A. Optic radiation lesion
- B. Lateral geniculate body lesion
- C. Optic tract lesion (Correct Answer)
- D. Anterior occipital cortex lesion
Explanation: ***Optic tract lesion*** - An **optic tract lesion** typically causes **incongruous homonymous hemianopia** because the fibers are not fully segregated by their retinal origin, leading to unequal visual field defects in the two eyes [1]. - The **Wernicke's hemianopic pupil** is a specific sign associated with optic tract lesions involving the afferent pupillary fibers, where direct light reflex is lost in the hemianopic half of the pupil, but consensual reflex is preserved [1]. *Optic radiation lesion* - An optic radiation lesion generally causes **congruous homonymous hemianopia**, as the fibers are more organized by retinal correspondence further along the visual pathway. - It does not typically present with a Wernicke's hemianopic pupil, as the pupillary fibers usually exit the visual pathway before reaching the optic radiations [1]. *Lateral geniculate body lesion* - A lesion of the lateral geniculate body (LGB) would result in a **congruous homonymous hemianopia**, similar to optic radiation lesions, because the fibers are already well-segregated and organized. - The LGB is primarily a relay station for visual information, and a lesion here would not typically affect the pupillary light reflex in the specific way seen in Wernicke's hemianopic pupil [1]. *Anterior occipital cortex lesion* - Lesions in the anterior occipital cortex, particularly the primary visual cortex, typically cause **macular sparing homonymous hemianopia** due to the dual blood supply to the macular representation area [1]. - Such lesions do not involve the afferent pupillary pathways and therefore would not cause a Wernicke's hemianopic pupil.
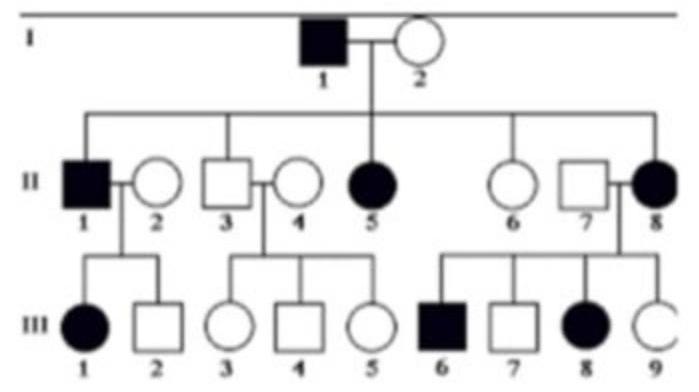
Question 27: 25-year-old man presents for a routine physical examination. The patient is tall and on examination, he was found to have an early diastolic murmur. His family pedigree is given below (image attached). Which of the following is the mode of inheritance by which the disease is likely to be transmitted?
- A. Autosomal Recessive
- B. X-Linked Recessive
- C. X-Linked Dominant
- D. Autosomal Dominant (Correct Answer)
Explanation: ***Autosomal Dominant*** - The pedigree shows that the disease appears in every generation, and affected individuals have at least one affected parent (e.g., I-1 passes it to II-1, II-5, II-8). This pattern is characteristic of **dominant inheritance**. - Both males and females are affected, and affected fathers can pass the trait to their sons (e.g., I-1 to II-1), ruling out X-linked inheritance and supporting an **autosomal dominant** mode. *Autosomal Recessive* - In autosomal recessive inheritance, affected individuals typically have **unaffected parents** (who are carriers), and the disease often skips generations. This is not observed in the provided pedigree. - While both males and females can be affected, the presence of affected individuals in every generation and vertical transmission makes recessive inheritance unlikely. *X-Linked Recessive* - X-linked recessive disorders typically show more affected males than females, and affected fathers **cannot pass the trait to their sons**. The pedigree clearly shows affected females and father-to-son transmission (I-1 to II-1 and potentially II-8 to III-6), ruling out this pattern. - Also, all daughters of an affected father would be carriers, and some an affected mother would have affected offspring. *X-Linked Dominant* - In X-linked dominant inheritance, all daughters of an affected father would be affected, and there is no male-to-male transmission. - The pedigree shows instances where affected fathers (like I-1) have unaffected daughters (e.g., II-2, II-4, II-6, II-7), and affected mothers (II-5, II-8) have unaffected children, which contradicts X-linked dominant inheritance.
Question 28: Renal tubular acidosis with ABG value pH = 7.24 PO2=80; PaCO2= 36 Na = 131; HCO3 = 14 Cl= 90; BE = -13 Glucose = 135 the above ABG picture suggests –
- A. Metabolic acidosis (Correct Answer)
- B. Respiratory alkalosis
- C. Metabolic alkalosis
- D. Respiratory acidosis
Explanation: The ABG shows a pH of 7.24, indicating **acidemia** [1]. The HCO3 is 14 mEq/L, which is significantly **low**, and the base excess (BE) is -13 [1]. The PaCO2 of 36 mmHg is within the normal range, indicating no significant primary respiratory derangement [2]. The overall picture is consistent with an uncompensated or partially compensated **metabolic acidosis** [1][2]. ***Metabolic acidosis*** - The **low pH (acidemia)**, **low bicarbonate (HCO3)**, and **negative base excess (BE)** are direct indicators of metabolic acidosis [1]. - The **PaCO2 within normal limits** or slightly decreased suggests either no respiratory compensation or insufficient compensation for the metabolic derangement [1][2]. *Respiratory acidosis* - This would present with a **low pH** and an **elevated PaCO2** as the primary defect, which is not seen here (PaCO2 is normal) [1]. - Bicarbonate would typically be normal or elevated if compensated, not significantly decreased. *Respiratory alkalosis* - This would be characterized by an **elevated pH** and a **low PaCO2**, which is the opposite of the findings in this ABG [1]. - HCO3 would be normal or low if compensated. *Metabolic alkalosis* - This would present with an **elevated pH** and an **elevated HCO3**, which contradicts the given ABG values (low pH and low HCO3) [2].
Question 29: What is the Child-Pugh class for a patient who has a serum bilirubin of 2.5 mg/dL, serum albumin of 3 g/dL, INR of 2, mild ascites, but no encephalopathy?
- A. Child-Pugh Class B (Correct Answer)
- B. Child-Pugh Class A
- C. Child-Pugh Class D
- D. Child-Pugh Class C
Explanation: ***Child-Pugh Class B*** - A serum bilirubin of **2.5 mg/dL** (2 points), serum albumin of **3 g/dL** (2 points), INR of **2** (2 points), and mild ascites (2 points), with no encephalopathy (1 point), sums up to a total of 9 points, which falls into the range for **Child-Pugh Class B** (7-9 points) [1]. - This class indicates **moderate hepatic dysfunction** and is characterized by a higher risk of complications and mortality compared to Class A. *Child-Pugh Class A* - This class is assigned for a total score of **5-6 points**, indicating **well-compensated hepatic disease**. - The patient's total score of 9 points exceeds the threshold for Class A, suggesting more significant liver impairment. *Child-Pugh Class D* - There is no Child-Pugh Class D; the classification system only includes classes A, B, and C. - This option is therefore incorrect based on the established Child-Pugh scoring system. *Child-Pugh Class C* - This class corresponds to a total score of **10-15 points**, indicative of **severe hepatic decompensation**. - The patient's calculated score of 9 points is below the minimum required for Child-Pugh Class C.
Question 30: Which of the following is associated with pauci-immune glomerulonephritis?
- A. Anti-GBM glomerulonephritis
- B. SLE nephritis
- C. IgA nephropathy
- D. Granulomatosis with polyangiitis (GPA) (Correct Answer)
Explanation: ***Granulomatosis with polyangiitis (GPA)*** - **Pauci-immune glomerulonephritis** is characterized by the absence or scarcity of immune complex deposits in the glomeruli. - This is typical of **ANCA-associated vasculitides**, such as GPA (formerly Wegener's granulomatosis), which cause severe necrotising glomerulonephritis with few immune deposits [1]. *Anti-GBM glomerulonephritis* - This condition is characterized by **linear deposition of anti-GBM antibodies** along the glomerular basement membrane, making it an **immune complex-mediated disease**, not pauci-immune [1]. - It involves autoantibodies attacking the **collagen type IV** in the GBM. *SLE nephritis* - Systemic lupus erythematosus (SLE) nephritis is a classic example of **immune complex-mediated glomerulonephritis**, with abundant immune deposits containing immunoglobulins and complement [1]. - The pathology often shows **full-house immunofluorescence** with IgG, IgA, IgM, C3, and C1q. *IgA nephropathy* - This is characterized by prominent **mesangial deposition of IgA immune complexes**, which is clearly an immune complex-mediated process [1]. - While it can present with different histological patterns, the presence of **IgA deposition** means it is not pauci-immune [1].