All SubjectsAnatomy (18)Anesthesiology (4)Biochemistry (26)Community Medicine (33)Dental (2)Dermatology (7)ENT (7)Forensic Medicine (13)Internal Medicine (54)Microbiology (21)Obstetrics and Gynecology (28)Ophthalmology (8)Orthopaedics (5)Pathology (25)Pediatrics (18)Pharmacology (27)Physiology (21)Psychiatry (9)Radiology (17)Surgery (23)
Q11
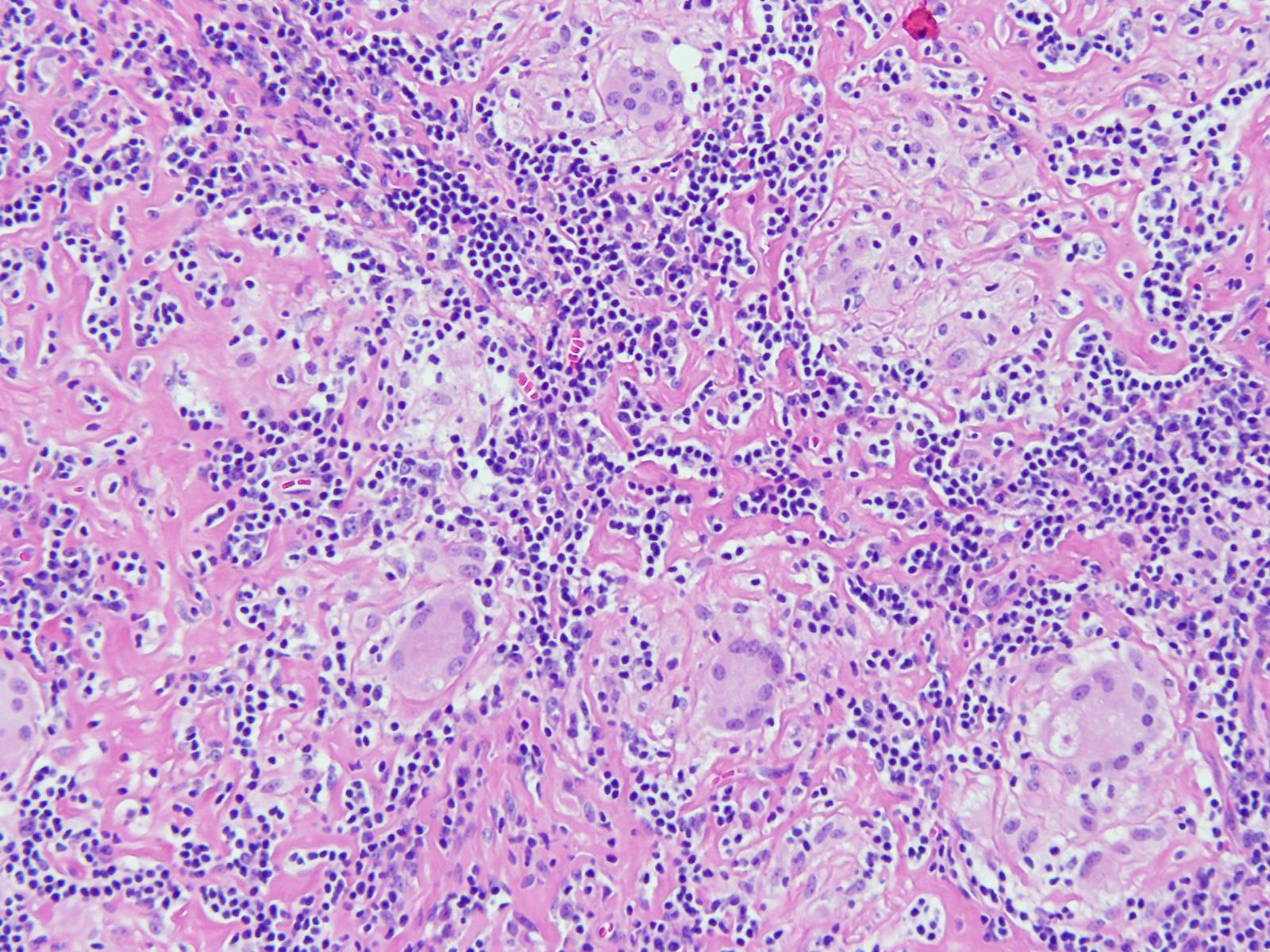
An 11-year-old boy presented with a cough for 15 days. On examination, he was found to have cervical lymphadenopathy. Lymph node biopsy showed the following findings. What could be the diagnosis?
Q12
Esophageal manometry was performed - it revealed panesophageal pressurization with distal contractile integrity as >450mm Hg pressure in the body. What will be the diagnosis?
Q13
Which is the most common pancreatic endocrine neoplasm?
Q14
The differentiating feature between IBS and organic GI disease is:
Q15
Screening is not useful in which carcinoma
Q16
Which of the following is commonly seen in Pituitary apoplexy?
Q17
A Patient falls down often with behavioral change and enuresis. What is the condition associated with him?
Q18
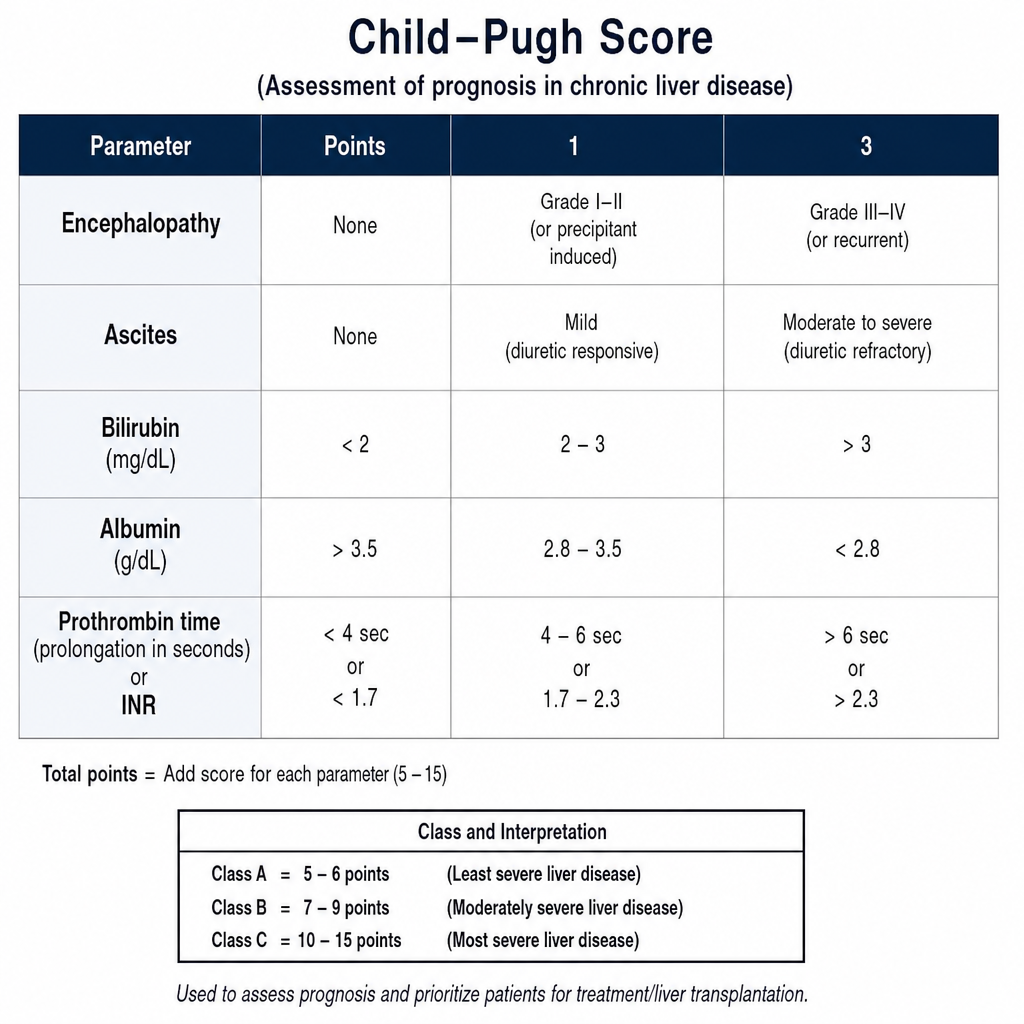
Which of the following criteria is used to assess the prognosis of liver conditions?
Q19
Renal tubular acidosis with ABG value pH = 7.24 PO2=80; PaCO2= 36 Na = 131; HCO3 = 14 Cl= 90; BE = -13 Glucose = 135 the above ABG picture suggests –
Q20
The patient is presenting with the deformity of the finger as shown. The PIP is involved but the DIP is spared
