NEET-PG 2020 — Anatomy
12 Previous Year Questions with Answers & Explanations
Which arch artery contributes to the formation of the aortic arch that influences the course of the left recurrent laryngeal nerve?
Identify the type of cartilage shown in the image.
The image shows a highlighted region on the dorsal aspect of the hand (anatomical snuffbox). Which of the following anatomical structures form the boundaries or floor of this region?

The patient is presenting with pain around the base of the thumb. Which tendons are likely involved?
Tumour of the uncinate process of the pancreas will compress which artery
Which of the following is a remnant of the Wolffian duct in females?
Identify the type of joint in the image provided.
Stimulation of the external auditory canal leads to cough due to which nerve?
The upward extension of thyroid swelling is prevented by which of the following structures
Episiotomy incision was extended posteriorly beyond perineal body injuring the structure immediately posterior to it. Which structure has been injured?
NEET-PG 2020 - Anatomy NEET-PG Practice Questions and MCQs
Question 1: Which arch artery contributes to the formation of the aortic arch that influences the course of the left recurrent laryngeal nerve?
- A. 4th arch (Correct Answer)
- B. 3rd arch
- C. 5th arch
- D. 2nd arch
Explanation: ***4th arch*** - The **left fourth aortic arch artery** gives rise to the **aortic arch** distal to the origin of the left subclavian artery. - The left recurrent laryngeal nerve hooks around the **ductus arteriosus** (a remnant of the 6th arch artery) and the aortic arch, making its course dependent on the development of the 4th aortic arch [1]. *3rd arch* - The **third aortic arch arteries** primarily contribute to the formation of the common carotid arteries and the proximal part of the internal carotid arteries. - These arteries are located superior to the structures that influence the recurrent laryngeal nerve's path. *5th arch* - The **fifth aortic arch arteries** are **rudimentary** or absent in humans. - They do not significantly contribute to the formation of major arterial structures in the adult, nor do they influence the recurrent laryngeal nerve. *2nd arch* - The **second aortic arch arteries** give rise to the stapedial arteries, which usually regress. - They are not involved in the formation of the great vessels in the mediastinum or the course of the recurrent laryngeal nerve.
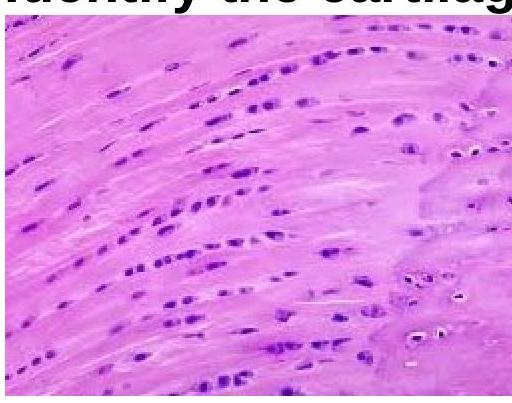
Question 2: Identify the type of cartilage shown in the image.
- A. Hyaline cartilage
- B. Elastic cartilage
- C. Dense connective tissue
- D. Fibrocartilage (Correct Answer)
Explanation: ***Fibrocartilage*** - The image displays **chondrocytes** arranged in rows between bundles of **collagen fibers**, characteristic of fibrocartilage. This structure provides high tensile strength and shock absorption. - Unlike other cartilage types, fibrocartilage lacks a distinct perichondrium and is found in structures requiring extreme strength, such as intervertebral discs and menisci. *Hyaline cartilage* - Hyaline cartilage has an amorphous, **glassy matrix** with chondrocytes typically arranged in small groups (isogenous groups) within lacunae, without prominent collagen bundles. - It is found in articular surfaces, tracheal rings, and the costal cartilages, providing smooth, low-friction surfaces. *Elastic cartilage* - Elastic cartilage is characterized by a high concentration of **elastic fibers** within its matrix, giving it flexibility and resilience. - Chondrocytes are typically scattered and the matrix stains darker due to the elastic fibers, which are not apparent in the image. *Dense connective tissue* - While dense connective tissue contains abundant **collagen fibers**, it lacks chondrocytes in lacunae, instead containing fibroblasts. - The presence of chondrocytes in the image confirms this is cartilage, not dense connective tissue.
Question 3: The image shows a highlighted region on the dorsal aspect of the hand (anatomical snuffbox). Which of the following anatomical structures form the boundaries or floor of this region?
- A. Abductor pollicis longus muscle.
- B. Styloid process of the radius.
- C. Extensor pollicis longus muscle.
- D. All of the above anatomical structures. (Correct Answer)
Explanation: ***All of the above anatomical structures.*** - The image highlights the **anatomical snuffbox**, a triangular depression on the radial dorsal aspect of the hand. Its boundaries are formed by the tendons of the **extensor pollicis longus muscle** (ulnar side), and the **abductor pollicis longus** and **extensor pollicis brevis muscles** (radial side). - The **styloid process of the radius** forms the floor of the anatomical snuffbox along with the scaphoid and trapezium bones. All the options listed are key anatomical features associated with this region. *Extensor pollicis longus muscle.* - This muscle forms the **ulnar (medial) border** of the anatomical snuffbox. - Its tendon can be palpated during **thumb extension** and contributes to the overall structure of the highlighted area. *Abductor pollicis longus muscle.* - This muscle, along with the extensor pollicis brevis, forms the **radial (lateral) border** of the anatomical snuffbox. - Its tendon is visible and palpable on the radial side of the highlighted region when the thumb is abducted. *Styloid process of the radius.* - This bony prominence is located at the **distal end of the radius** on the radial side of the wrist. - It forms part of the **proximal floor** of the anatomical snuffbox, contributing to its definition.
Question 4: The patient is presenting with pain around the base of the thumb. Which tendons are likely involved?
- A. APB & EPL
- B. APL & EPB (Correct Answer)
- C. APB & EPB
- D. APL & EPL
Explanation: ***APL & EPB*** - Pain around the base of the thumb, especially with movement, is characteristic of De Quervain's tenosynovitis [1]. This condition involves the **abductor pollicis longus (APL)** and **extensor pollicis brevis (EPB)** tendons [1]. - These two tendons share a common synovial sheath as they pass through the first dorsal compartment of the wrist, making them susceptible to inflammation and friction [1]. *APB & EPL* - **APB (Abductor Pollicis Brevis)** is an intrinsic hand muscle found in the thenar eminence, primarily involved in thumb abduction, and is not typically associated with De Quervain's tenosynovitis. - **EPL (Extensor Pollicis Longus)** is part of the third dorsal compartment and its tendon crosses over the other thumb tendons, and is not inflamed in De Quervain's tenosynovitis. *APB & EPB* - As mentioned, **APB (Abductor Pollicis Brevis)** is an intrinsic hand muscle, not involved in De Quervain's tenosynovitis. - While **EPB (Extensor Pollicis Brevis)** is involved, its combination with APB incorrectly identifies the primary tendons affected in the first dorsal compartment. *APL & EPL* - **APL (Abductor Pollicis Longus)** is one of the correct tendons involved. - **EPL (Extensor Pollicis Longus)** belongs to the third dorsal compartment of the wrist and is not typically affected in De Quervain's tenosynovitis, differentiating it from the tendons in the first dorsal compartment [1].
Question 5: Tumour of the uncinate process of the pancreas will compress which artery
- A. Superior mesenteric artery (Correct Answer)
- B. Inferior mesenteric artery
- C. Common hepatic artery
- D. Splenic artery
Explanation: ***Superior mesenteric artery*** - The **uncinate process** forms the lower and medial part of the head of the pancreas, hooking around and behind the **superior mesenteric vessels**. - A tumor in this region would therefore almost immediately compress the **superior mesenteric artery** and vein due to its close anatomical relationship. *Splenic artery* - The **splenic artery** runs along the superior border of the pancreas, primarily associated with the body and tail. - A tumor in the **uncinate process** (part of the head) would be anatomically distant from the splenic artery, making compression unlikely. *Inferior mesenteric artery* - The **inferior mesenteric artery** arises from the aorta much lower than the pancreas, typically at the L3 vertebral level. - Its anatomical position makes it spatially separated from the uncinate process of the pancreas, so compression is not expected. *Common hepatic artery* - The **common hepatic artery** runs anterior to the portal vein and to the left of the bile duct, supplying the liver. - It is located superior to the head of the pancreas and away from the uncinate process, hence not typically affected by tumors in that specific pancreatic region.
Question 6: Which of the following is a remnant of the Wolffian duct in females?
- A. Pouch of Douglas
- B. Uterovesical pouch
- C. Gartner’s cyst (Correct Answer)
- D. Broad ligament
Explanation: ***Gartner’s cyst*** - **Gartner's cysts** are remnants of the **Wolffian duct (mesonephric duct)** in females [3]. These ducts normally regress in females but can persist as vestigial structures [3]. - They typically present as cysts or small ducts along the lateral walls of the vagina or in the broad ligament [2], [3]. *Pouch of Douglas* - The **Pouch of Douglas (rectouterine pouch)** is a peritoneal recess located between the rectum and the uterus, not a remnant of the Wolffian duct [2]. - It is formed during development as the peritoneum drapes over the pelvic organs. *Uterovesical pouch* - The **uterovesical pouch** is a peritoneal reflection located between the uterus and the bladder, separate from the Wolffian duct remnants [1]. - Like the Pouch of Douglas, it is a normal anatomical space formed by the arrangement of the peritoneum in the pelvis. *Broad ligament* - The **broad ligament** is a wide fold of peritoneum that supports the uterus, fallopian tubes, and ovaries. It is not a remnant of the Wolffian duct itself, though Wolffian duct remnants (like Gartner's ducts) can sometimes be found within it [3]. - It serves as a mesentery for the reproductive organs, connecting them to the lateral walls of the pelvis.
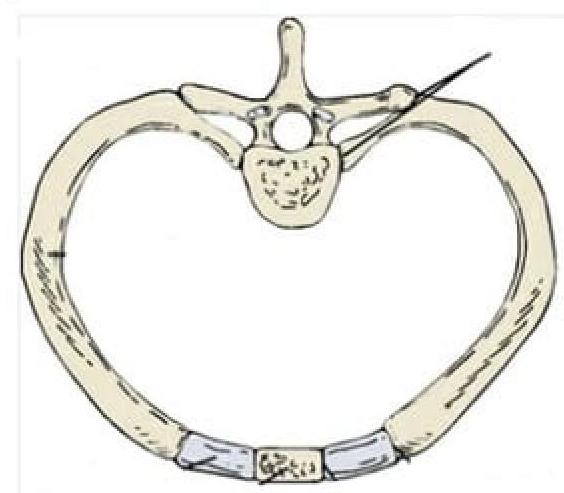
Question 7: Identify the type of joint in the image provided.
- A. Syndesmosis
- B. Synarthrosis
- C. Synovial joint (Correct Answer)
- D. Symphysis
Explanation: ***Synovial joint*** - The image depicts a **costovertebral joint**, which connects a rib to a thoracic vertebra. These joints are **diarthrotic**, meaning they are freely movable, characteristic of synovial joints. - Synovial joints are characterized by the presence of a **synovial cavity**, articular cartilage, an articular capsule, and synovial fluid, allowing for a wide range of motion. *Syndesmosis* - A syndesmosis is a type of **fibrous joint** where two bones are joined by a ligament or a membrane, allowing for very limited movement, such as the distal tibiofibular joint. - This definition does not match the image, which shows a joint designed for movement between the rib and vertebra. *Synarthrosis* - Synarthrosis is a classification for **immovable joints**, such as sutures in the skull. - The costovertebral joints, as shown, allow for movement during respiration and are therefore not synarthrotic. *Symphysis* - A symphysis is a type of **cartilaginous joint** where bones are joined by **fibrocartilage**, allowing for slight movement. Examples include the pubic symphysis or intervertebral discs. - The costovertebral joint shown in the image is a synovial articulation, not a cartilaginous joint.
Question 8: Stimulation of the external auditory canal leads to cough due to which nerve?
- A. Auricular branch of vagus (Correct Answer)
- B. Greater auricular nerve
- C. Auriculotemporal nerve
- D. Facial Nerve
Explanation: ***Auricular branch Vagus*** - The **auricular branch of the vagus nerve (Arnold's nerve)** innervates the posterior and inferior walls of the external auditory canal. - Stimulation of this nerve can trigger the **cough reflex**, as the vagus nerve is also responsible for innervating the larynx, pharynx, and trachea. *Greater auricular nerve* - The **greater auricular nerve** is a cutaneous nerve from the cervical plexus (C2-C3) that supplies sensation to the skin over the mastoid process, posterior auricle, and part of the earlobe. - It does not directly innervate the external auditory canal in a way that would trigger a cough reflex. *Auriculotemporal nerve* - The **auriculotemporal nerve** is a branch of the mandibular nerve (V3) that provides sensory innervation to the temporomandibular joint, skin over the temple, and part of the external ear. - While it innervates part of the ear, its stimulation does not typically elicit a cough reflex. *Facial Nerve* - The **facial nerve** is primarily responsible for motor innervation of the muscles of facial expression and taste sensation to the anterior two-thirds of the tongue. - Although it has a small sensory component to the external ear (via auricular branches), it is not the primary nerve responsible for the cough reflex when the external auditory canal is stimulated.
Question 9: The upward extension of thyroid swelling is prevented by which of the following structures
- A. Sternothyroid
- B. Thyrohyoid membrane
- C. Ligament of berry
- D. Pretracheal fascia (Correct Answer)
Explanation: ***Pretracheal fascia*** - The **pretracheal fascia** is a deep cervical fascia layer that **envelops the thyroid gland** and is continuous with the fibrous capsule of the gland. - Due to its attachments, particularly to the **cricoid cartilage** and **recurrent laryngeal nerve sheath**, it anchors the thyroid gland and **restricts its upward movement** during swallowing. *Sternothyroid* - The **sternothyroid muscle** depresses the larynx and thyroid gland, but it does **not inherently prevent upward extension** of a thyroid swelling. - Its action is on the **movement of the larynx** and thyroid, rather than an anatomical barrier to swelling. *Thyrohyoid membrane* - The **thyrohyoid membrane** connects the thyroid cartilage to the hyoid bone and allows for movement between them, but it has no direct role in **preventing upward extension of a thyroid swelling**. - It is mainly involved in **laryngeal elevation** during swallowing. *Ligament of Berry* - The **ligament of Berry** (or lateral suspensory ligament) connects the thyroid gland to the **cricoid cartilage** and **trachea** [1]. - While it offers some stability to the thyroid gland, its primary role is to **anchor the gland posteriorly** rather than prevent the upward extension of a swelling [1].
Question 10: Episiotomy incision was extended posteriorly beyond perineal body injuring the structure immediately posterior to it. Which structure has been injured?
- A. External anal sphincter (Correct Answer)
- B. Ischiocavernosus
- C. Urethral sphincter
- D. Bulbospongiosus
Explanation: ***External anal sphincter*** - An overextended **episiotomy incision** that goes beyond the perineal body posteriorly will likely injure the **external anal sphincter**, which is immediately posterior to the perineal body [4]. - Injury to this sphincter can lead to **fecal incontinence** [1]. *Ischiocavernosus* - The **ischiocavernosus muscle** is located more laterally in the perineum and plays a role in clitoral erection, not directly posterior to the perineal body. - An episiotomy extending posteriorly would not typically involve this muscle. *Urethral sphincter* - The **urethral sphincter** is located anterior to the perineal body and surrounds the urethra [3]. - Injury to this sphincter is associated with anterior perineal trauma, not posterior extension of an episiotomy [3]. *Bulbospongiosus* - The **bulbospongiosus muscle** is a superficial perineal muscle that surrounds the vaginal orifice and contributes to the perineal body [4]. - While it can be involved in an episiotomy, the structure immediately posterior to the perineal body itself is the external anal sphincter [2].