All SubjectsAnatomy (167)Anesthesiology (9)Biochemistry (108)Community Medicine (87)Dental (8)Dermatology (19)ENT (30)Forensic Medicine (62)General Medicine (3)Internal Medicine (136)Microbiology (101)Obstetrics and Gynecology (65)Ophthalmology (60)Orthopaedics (33)Pathology (107)Pediatrics (37)Pharmacology (123)Physiology (116)Psychiatry (2)Psychiatry (38)Radiology (25)Surgery (81)
Q11
Investigation of choice for acute intracerebral hemorrhage is -
Q12
Investigation of choice to evaluate intracranial hemorrhage of less than 48 hours is -
Q13
Cobra head appearance on excretory urography is suggestive of?
Q14
On CT chest, the 'halo sign' is particularly associated with which condition in immunocompromised patients?
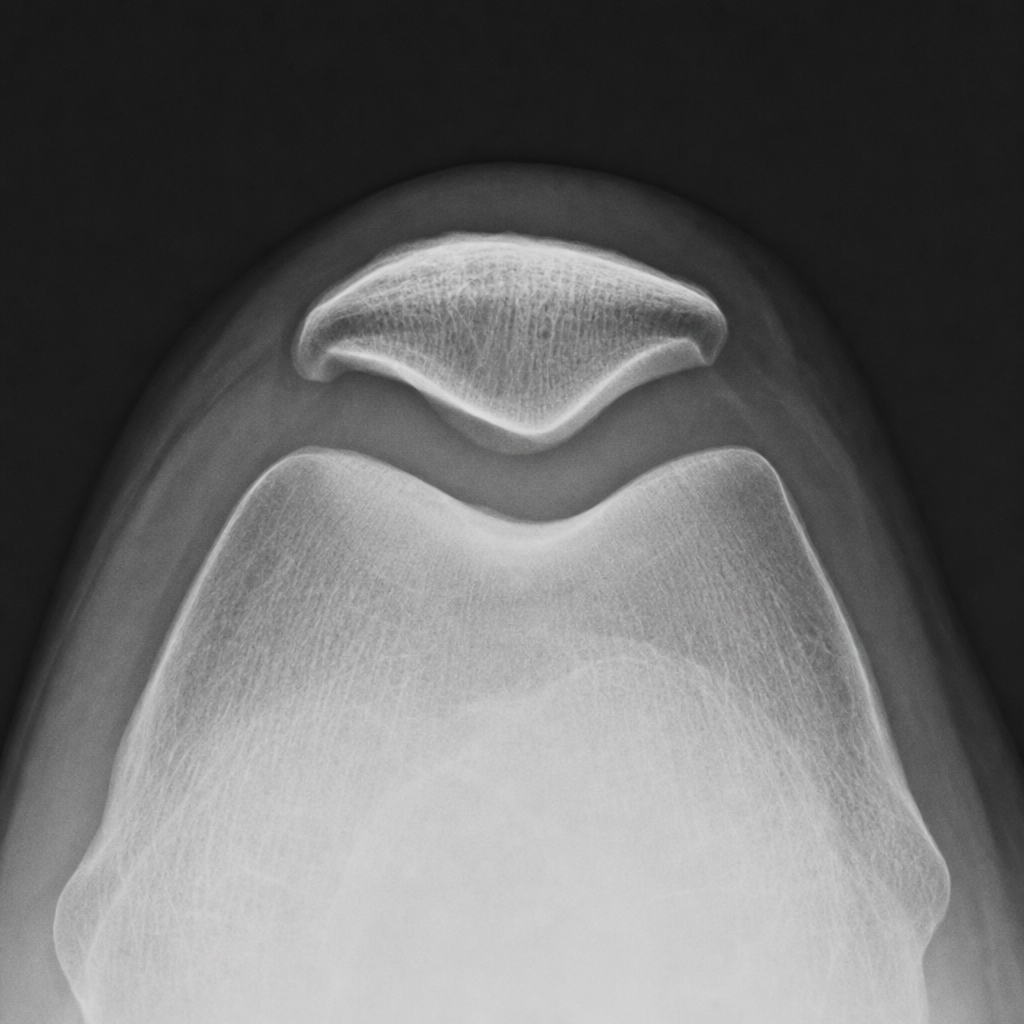
Q15
What condition is best diagnosed using a Skyline view X-ray?
Q16
Which of the following statements about lipoma is radiologically true?
Q17
Epidural hematoma on CT scan shows which of the following?
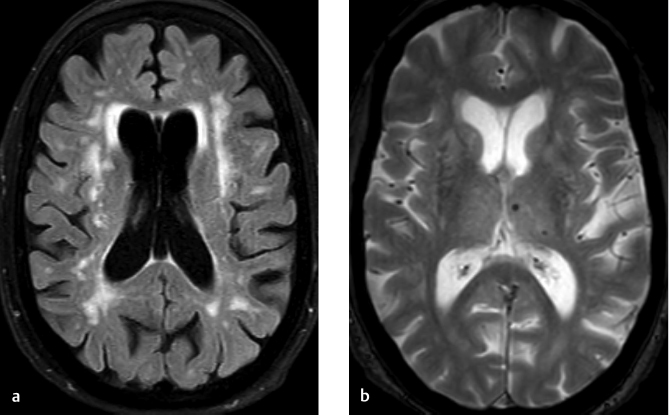
Q18
Tigroid pattern on MRI is seen in -
Q19
Which of the following X-ray findings is associated with Chilaiditi syndrome?
Q20
Investigation of choice for soft tissue sarcoma is -