All (1417)Anatomy (167)Anesthesiology (9)Biochemistry (108)Community Medicine (87)Dental (8)Dermatology (19)ENT (30)Forensic Medicine (62)General Medicine (3)Internal Medicine (136)Microbiology (101)Obstetrics and Gynecology (65)Ophthalmology (60)Orthopaedics (33)Pathology (107)Pediatrics (37)Pharmacology (123)Physiology (116)Psychiatry (2)Psychiatry (38)Radiology (25)Surgery (81)
Q291
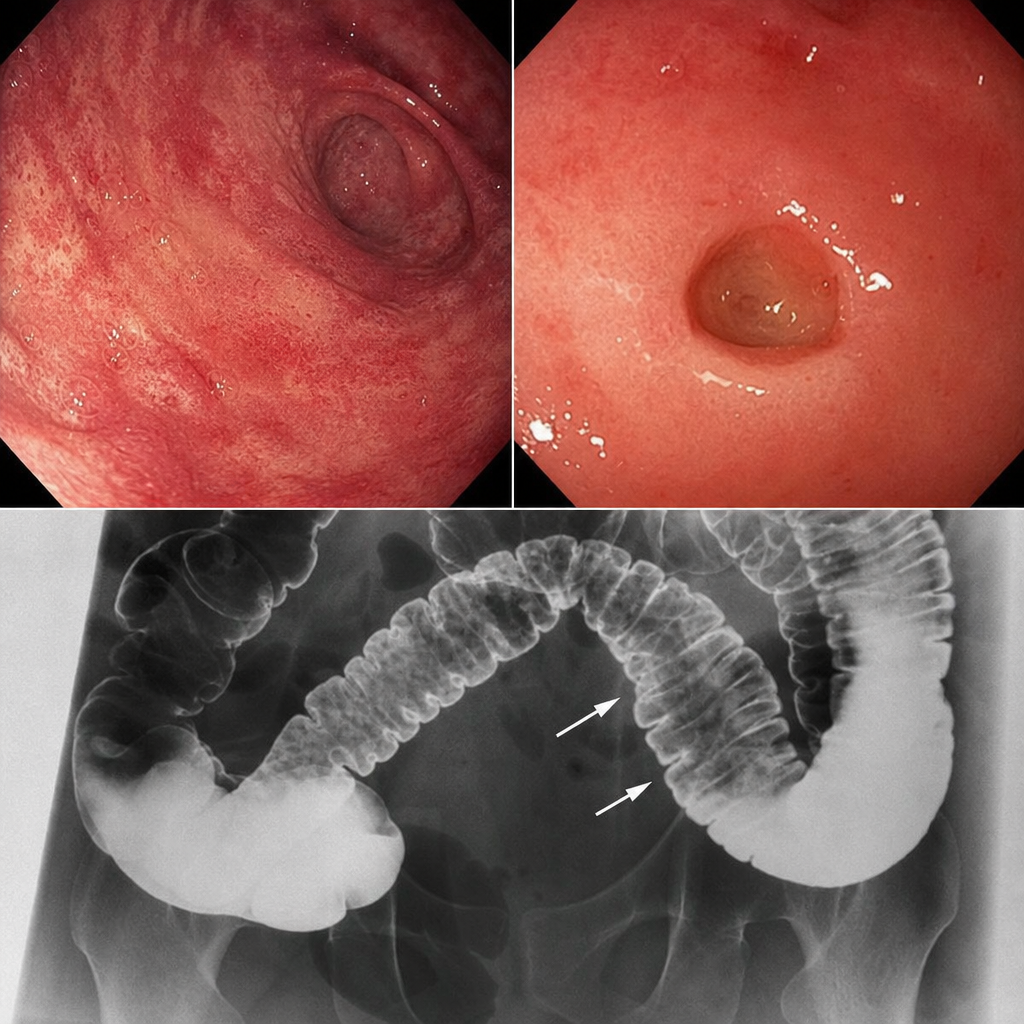
A patient presents with skin involvement and collar stud ulceration in the intestine observed on radiography. What is the most likely diagnosis?