INI-CET 2024 — Radiology
5 Previous Year Questions with Answers & Explanations
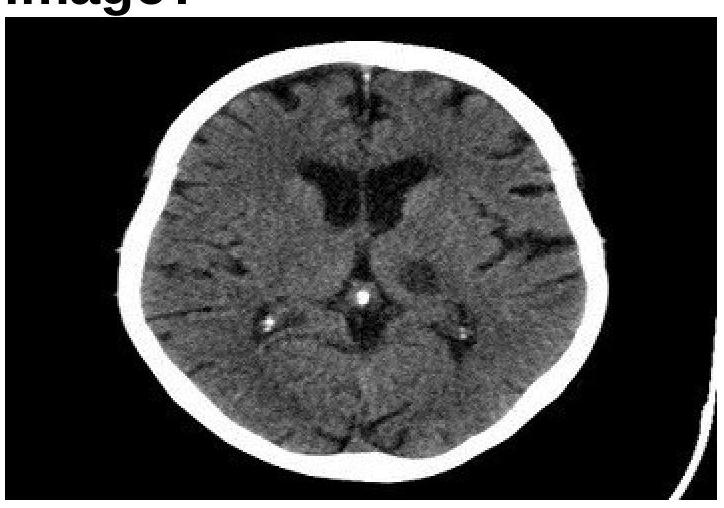
Identify the condition in the image below?
Which of the following statements about CT imaging is the MOST accurate?
Which sign on chest X-ray indicates tension pneumothorax?
X-ray chest in a neonate may show 'ground glass' haziness in all the following conditions EXCEPT:
Which of the following contrast agents is PREFERRED in a patient with renal dysfunction for the prevention of contrast-induced nephropathy?
INI-CET 2024 - Radiology INI-CET Practice Questions and MCQs
Question 1: Identify the condition in the image below?
- A. Lacunar infarct (Correct Answer)
- B. Embolic infarct
- C. Thrombotic infarct
- D. Intracerebral hemorrhage
Explanation: ***Lacunar infarct*** - The image displays a small, well-demarcated **hypodensity** (darker area) in the basal ganglia region, characteristic of a lacunar infarct. - Lacunar infarcts are typically caused by **occlusion of small perforating arteries** and result in small, deep infarcts, often appearing as precise, round or ovoid lesions on CT. *Embolic infarct* - Embolic infarcts tend to be **larger**, wedge-shaped, and often extend to the cortical surface, unlike the deep, small lesion seen. - They are commonly associated with a **cardiac source** or large artery atherosclerosis leading to distal embolization. *Thrombotic infarct* - Thrombotic infarcts are usually **larger** areas of infarction due to occlusion of a major artery, often preceded by symptoms like TIAs. - While they also appear hypodense, they are typically **more extensive** and less precisely defined than a lacunar infarct in the early stages. *Intracerebral hemorrhage* - Intracerebral hemorrhage would appear as a **hyperdense** (bright white) area on a non-contrast CT scan due to the presence of acute blood. - The image clearly shows a **hypodense lesion**, ruling out acute hemorrhage.
Question 2: Which of the following statements about CT imaging is the MOST accurate?
- A. Water has a Hounsfield unit (HU) of zero. (Correct Answer)
- B. CT head dose remains constant regardless of the protocol used.
- C. CT cannot detect gallstones under any circumstances.
- D. CT uses unfiltered x-ray beams.
Explanation: ***Water has a Hounsfield unit (HU) of zero.*** - The **Hounsfield unit (HU)** scale is a quantitative scale used to describe radiodensity in CT scans, where **water is defined as 0 HU**. - This establishes a crucial reference point for measuring the attenuation of other tissues, which can range from approximately **-1000 HU for air** to **+1000 HU or more for dense bone**. *CT head dose remains constant regardless of the protocol used.* - The **radiation dose** in CT scans is highly variable and depends significantly on the **protocol used**, including factors like mA, kVp, pitch, and scan length. - **Dose optimization techniques** and protocol adjustments are routinely employed to minimize patient exposure while maintaining diagnostic image quality. *CT cannot detect gallstones under any circumstances.* - While **ultrasound (US)** is the primary modality for detecting gallstones, CT can visualize them, especially if they are **calcified** or of mixed composition. - **Non-calcified gallstones** may be more challenging to detect on CT, but they are not impossible to see, particularly with current generation scanners and appropriate windowing. *CT uses unfiltered x-ray beams.* - CT scanners use **filtered x-ray beams** to provide higher quality images and reduce patient dose. - **Filtration (e.g., aluminum or copper)** removes low-energy x-rays, which would otherwise be absorbed by the patient without contributing to image formation.
Question 3: Which sign on chest X-ray indicates tension pneumothorax?
- A. Mediastinal shift (Correct Answer)
- B. Flattened diaphragm
- C. Deep sulcus sign
- D. All of the options
Explanation: ***Mediastinal shift*** - **Mediastinal shift** away from the affected side is the **most specific and critical radiographic sign** of tension pneumothorax on chest X-ray. - The progressive air accumulation under positive pressure pushes the **mediastinum** (heart, great vessels, trachea) toward the contralateral side, causing life-threatening **cardiorespiratory compromise** by impeding venous return and cardiac output. - This finding distinguishes tension pneumothorax from simple pneumothorax and mandates **immediate needle decompression**. *Flattened diaphragm* - A **flattened or depressed hemidiaphragm** can occur in tension pneumothorax due to increased intrapleural pressure pushing the diaphragm downward. - However, this sign is **non-specific** as it also occurs in simple pneumothorax, hyperinflation, COPD, and other conditions. - While supportive, it does not definitively indicate the high-pressure tension state. *Deep sulcus sign* - The **deep sulcus sign** (abnormally deep and lucent costophrenic angle) is seen on **supine chest X-rays** when air accumulates anteriorly and inferiorly in the pleural space. - This indicates pneumothorax but is **not specific for tension pneumothorax** and can be seen in simple pneumothorax. - It is position-dependent and does not indicate mediastinal compression. *All of the options* - While flattened diaphragm and deep sulcus sign **may be present** in tension pneumothorax, only **mediastinal shift** is the **definitive radiographic indicator** that distinguishes tension from simple pneumothorax. - Mediastinal shift is the key finding that reflects the pathophysiological pressure differential causing cardiovascular compromise.
Question 4: X-ray chest in a neonate may show 'ground glass' haziness in all the following conditions EXCEPT:
- A. Left-to-right shunt (Correct Answer)
- B. Obstructed TAPVC
- C. Staphylococcal pneumonia
- D. Hyaline membrane disease
Explanation: ***Left-to-right shunt*** - A **left-to-right shunt** in a neonate typically causes an increase in pulmonary blood flow, leading to vascular congestion and possibly **cardiomegaly**, not ground-glass haziness. - While prolonged significant shunting can lead to pulmonary edema, classic "ground glass" haziness is more characteristic of diffuse lung pathology. *Obstructed TAPVC* - **Obstructed total anomalous pulmonary venous connection (TAPVC)** leads to severe pulmonary venous congestion, resulting in **pulmonary edema** and a classic **ground-glass appearance** on chest X-ray. - This condition is a surgical emergency due to severe respiratory distress and lung opacification. *Staphylococcal pneumonia* - **Staphylococcal pneumonia** in neonates can cause extensive **pulmonary inflammation** and **exudate formation**, leading to a diffuse alveolar filling pattern that appears as ground-glass opacities. - This is a severe form of pneumonia that can rapidly progress. *Hyaline membrane disease* - **Hyaline membrane disease (respiratory distress syndrome)** is characterized by surfactant deficiency, leading to diffuse **atelectasis** and **pulmonary edema**, which manifests as a **ground-glass appearance** on chest X-ray. - This condition commonly affects premature infants and is associated with air bronchograms.
Question 5: Which of the following contrast agents is PREFERRED in a patient with renal dysfunction for the prevention of contrast-induced nephropathy?
- A. Iso-osmolar contrast (Correct Answer)
- B. High osmolar contrast
- C. Ionic contrast
- D. Low osmolar contrast
Explanation: ***Iso-osmolar contrast*** - **Iso-osmolar contrast agents** (e.g., iodixanol) have an osmolality of ~290 mOsm/kg, which is identical to that of plasma. - **This is the PREFERRED choice** in patients with renal dysfunction as multiple studies demonstrate the lowest risk of contrast-induced nephropathy (CIN). - The iso-osmolar formulation minimizes osmotic stress on renal tubules and reduces the risk of acute kidney injury. - **Current guidelines recommend iso-osmolar agents as first-line** in high-risk patients with pre-existing renal impairment. *Low osmolar contrast* - **Low osmolar contrast agents** have osmolality of 600-900 mOsm/kg, which is significantly lower than high osmolar agents but still 2-3 times higher than plasma. - While **acceptable and safer than high osmolar agents**, they are not as optimal as iso-osmolar contrast for patients with renal dysfunction. - These agents are widely used and represent a reasonable alternative when iso-osmolar agents are not available. *High osmolar contrast* - **High osmolar contrast agents** have osmolality >1400 mOsm/kg (about 5 times that of plasma). - They carry the **highest risk of contrast-induced nephropathy** due to severe osmotic load and direct tubular toxicity. - **Contraindicated or strongly avoided** in patients with pre-existing renal dysfunction. *Ionic contrast* - **Ionic contrast** refers to the chemical structure (dissociates into ions) rather than osmolality. - Can be either high or low osmolar—the ionic nature alone does not determine renal safety. - The critical factor for nephrotoxicity prevention is osmolality, not ionic charge.