INI-CET 2024 — Internal Medicine
23 Previous Year Questions with Answers & Explanations
All of the following can occur in rheumatic fever except?
What is the mode of inheritance for the most common form of hypophosphatemic rickets?
An 11-year-old boy presented with a cough for 15 days. On examination, he was found to have cervical lymphadenopathy. Lymph node biopsy showed the following findings. What could be the diagnosis?
Which of the following is a known risk factor for cholangiocarcinoma?
In folate deficiency, which of the following statements is true?
A male patient with purple striae, thin skin, non-healing wound, and pedunculated abdomen, most probable cause?
A 20-year-old chronic alcoholic presents with severe hematemesis. USG shows distension of portal vein and the liver appears hyperechoic. Pantoprazole has been initiated. What is the next step in management?
Which of the following statements about atrial fibrillation is correct?
A patient presents with the following arterial blood gas (ABG) and electrolyte values: pH: 7.34, Na: 135 mEq/L, Cl: 93 mEq/L, HCO3: 20 mEq/L, Random Blood Sugar (RBS): 420 mg/dl. What is the most likely acid-base disturbance?
Which of the following is not a complication of hypokalemia?
INI-CET 2024 - Internal Medicine INI-CET Practice Questions and MCQs
Question 1: All of the following can occur in rheumatic fever except?
- A. Mitral regurgitation
- B. Mitral stenosis
- C. Pericarditis
- D. Tricuspid regurgitation as the primary valve lesion (Correct Answer)
Explanation: ***Tricuspid regurgitation as the primary valve lesion*** - While **rheumatic fever** can affect any heart valve, the **tricuspid valve** is rarely affected as the **primary or sole lesion**. - It is most commonly seen in conjunction with more severe **mitral and aortic valve disease**. *Mitral regurgitation* - **Mitral regurgitation** is a common manifestation of **acute rheumatic fever**, occurring due to **inflammation** of the valve leaflets and **chordae tendineae** [1]. - This leads to incompetence of the valve, causing blood to flow back into the left atrium during systole [1]. *Mitral stenosis* - **Mitral stenosis** is a classic **long-term complication** of **rheumatic fever**, typically developing years to decades after the initial acute episode. - Repeated inflammation and scarring lead to **thickening and fusion of the mitral valve leaflets**, restricting blood flow. *Pericarditis* - **Pericarditis**, inflammation of the **pericardium** (the sac surrounding the heart), is a possible manifestation of **rheumatic carditis** in acute rheumatic fever [1]. - It can cause chest pain and may be accompanied by a **pericardial effusion** [1].
Question 2: What is the mode of inheritance for the most common form of hypophosphatemic rickets?
- A. Autosomal Recessive (AR)
- B. Autosomal Dominant (AD)
- C. X-Linked Recessive (XR)
- D. X-Linked Dominant (XD) (Correct Answer)
Explanation: ***X-Linked Dominant (XD)*** - The most common form of hypophosphatemic rickets is **X-linked hypophosphatemic rickets (XLH)**, which is inherited in an X-linked dominant pattern. - This condition is caused by mutations in the **PHEX gene** on the X chromosome, leading to impaired phosphate reabsorption in the kidneys. *Autosomal Recessive (AR)* - While some rare forms of hypophosphatemic rickets exist with **autosomal recessive** inheritance, they are not the most common. - These forms typically involve mutations in genes affecting phosphate transport or vitamin D metabolism, distinct from the primary defect in XLH. *Autosomal Dominant (AD)* - There are also rare **autosomal dominant** forms of hypophosphatemic rickets, such as hereditary hypophosphatemic rickets with hypercalciuria (HHRH) or autosomal dominant hypophosphatemic rickets (ADHR). - However, these are less common than the X-linked dominant form (XLH). *X-Linked Recessive (XR)* - **X-linked recessive** inheritance typically affects males more severely and exclusively, with carrier females usually unaffected or mildly affected. - In X-linked dominant conditions like XLH, both males and females are affected, though females may exhibit variable expressivity.
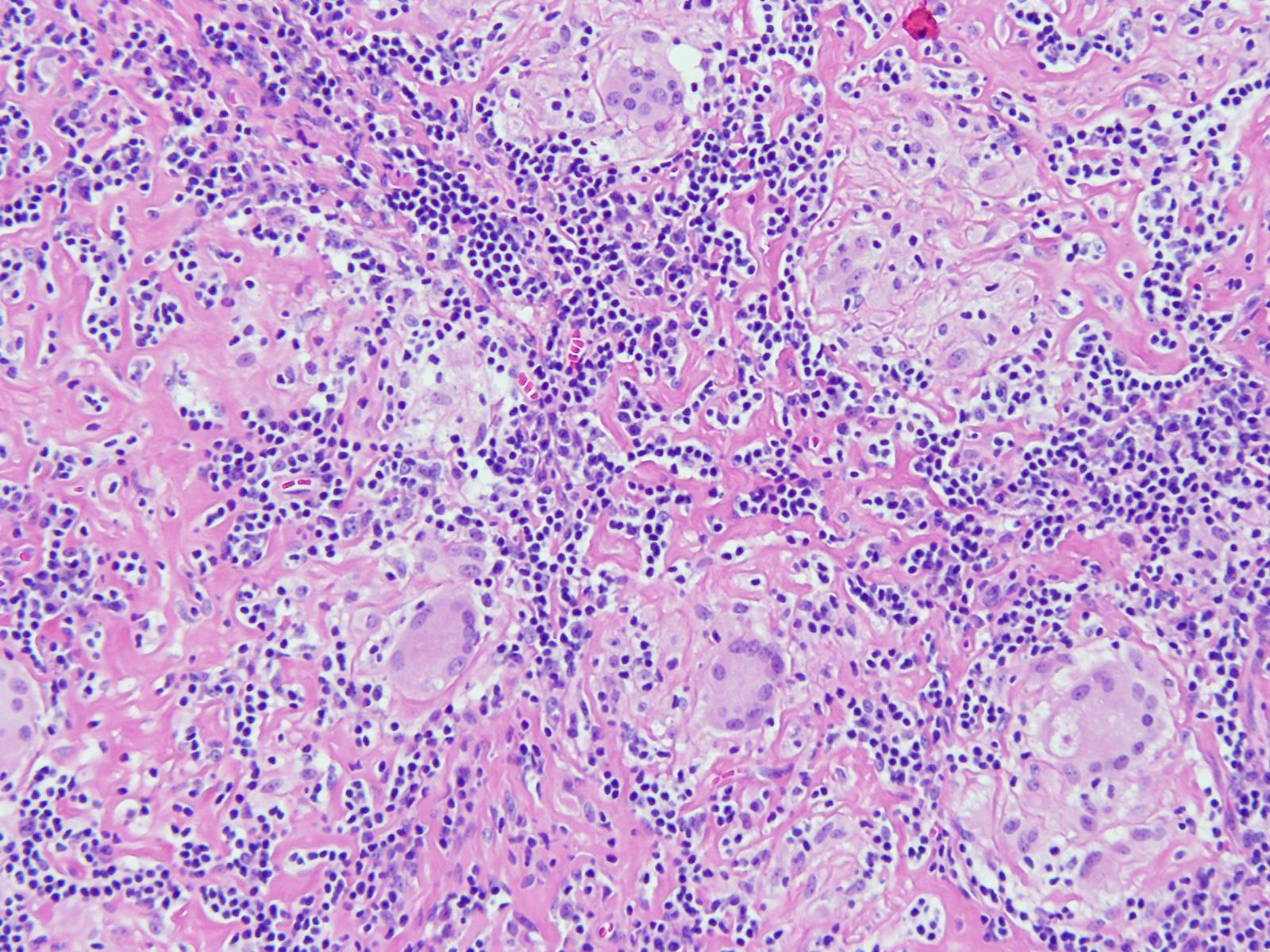
Question 3: An 11-year-old boy presented with a cough for 15 days. On examination, he was found to have cervical lymphadenopathy. Lymph node biopsy showed the following findings. What could be the diagnosis?
- A. Leprosy
- B. Sarcoidosis
- C. Syphilis
- D. Tuberculosis (Correct Answer)
Explanation: ***Tuberculosis*** - The image likely displays **granulomatous inflammation** with **caseous necrosis**, which is highly characteristic of **tuberculosis**, especially in someone presenting with a persistent cough and lymphadenopathy. - The presence of **cervical lymphadenopathy** along with a **cough** for 15 days in an 11-year-old boy points towards extrapulmonary tuberculosis or primary tuberculosis infection affecting the mediastinal lymph nodes with cervical involvement. *Leprosy* - While leprosy also causes granulomas, it typically manifests as skin lesions and nerve involvement, and lymphadenopathy is less common or specific as the primary initial presentation. - The granulomas in leprosy are often **epithelioid** with **foamy histiocytes** and numerous acid-fast bacilli, which are not explicitly described or obvious in the provided context for a definitive diagnosis without special stains. *Sarcoidosis* - Sarcoidosis involves **non-caseating granulomas**, meaning there is no central necrosis, which is a key differentiating feature from the caseating necrosis often seen in tuberculosis. - Although sarcoidosis can cause lymphadenopathy and cough, the microscopic features in the image, particularly if showing necrosis, would argue against sarcoidosis. *Syphilis* - Syphilis can cause lymphadenopathy (especially in secondary syphilis), but the characteristic histological finding is usually a **plasma cell-rich infiltrate** with **endarteritis obliterans**, not typically prominent granulomas with caseous necrosis. - Clinical presentation with cough and chronic lymphadenopathy in an 11-year-old would also make syphilis a less likely primary consideration without other suggestive signs.
Question 4: Which of the following is a known risk factor for cholangiocarcinoma?
- A. Giardia lamblia (intestinal protozoa) infection
- B. Ascaris lumbricoides (roundworm) infection
- C. Clonorchis sinensis infestation (Correct Answer)
- D. Paragonimus westermani infestation
Explanation: ***Clonorchis sinensis infestation*** - **Clonorchis sinensis**, also known as the Chinese liver fluke, is a well-established and significant risk factor for the development of **cholangiocarcinoma**. - Chronic inflammation and irritation of the bile ducts caused by the parasite are believed to promote malignant transformation. *Giardia lamblia (intestinal protozoa) infection* - **Giardia lamblia** is a common intestinal parasite causing giardiasis, characterized by diarrhea and malabsorption. - While it affects the gastrointestinal tract, there is **no known association** between *Giardia* infection and an increased risk of cholangiocarcinoma. *Paragonimus westermani infestation* - **Paragonimus westermani** is a lung fluke that primarily causes paragonimiasis, affecting the lungs and leading to cough and hemoptysis. - This parasite is not associated with direct bile duct inflammation or an increased risk of **cholangiocarcinoma**. *Ascaris lumbricoides (roundworm) infection* - **Ascaris lumbricoides** is a large intestinal roundworm that can cause intestinal obstruction or nutrient deficiencies. - Although it can occasionally migrate into the biliary tree, it is **not considered a risk factor** for cholangiocarcinoma [1].
Question 5: In folate deficiency, which of the following statements is true?
- A. B12 supplementation is recommended along with folate
- B. Purine and pyrimidine synthesis are affected
- C. Hemolytic anemia is not a feature
- D. Elevated homocysteine & normal methylmalonic acid (Correct Answer)
Explanation: ***Elevated homocysteine & normal methylmalonic acid*** - In **folate deficiency**, the conversion of homocysteine to methionine is impaired, leading to **elevated homocysteine** levels. - Unlike vitamin B12 deficiency, **methylmalonic acid (MMA)** levels remain normal in folate deficiency because folate is not involved in its metabolism. *B12 supplementation is recommended along with folate* - Supplementation with B12 alongside folate is crucial when **macrocytic anemia** is diagnosed, as it can mask a coexisting **B12 deficiency**, potentially worsening neurological symptoms if only folate is given. - However, in confirmed isolated folate deficiency, B12 supplementation is not strictly necessary unless there is suspicion or diagnosis of co-existing B12 deficiency. *Purine and pyrimidine synthesis are affected* - While folate is essential for **DNA synthesis**, indirectly affecting purine and pyrimidine production, this statement is a consequence rather than the primary diagnostic or distinguishing feature of folate deficiency. - **Folate** acts as a coenzyme in transferring one-carbon units, vital for the synthesis of **thymidylate** (a pyrimidine base) and **purine precursors**. *Hemolytic anemia is not a feature* - **Hemolytic anemia** is not typically a feature of folate deficiency; instead, it is characterized by **macrocytic, megaloblastic anemia**. - Conditions like **glucose-6-phosphate dehydrogenase (G6PD) deficiency** or **autoimmune disorders** are commonly associated with hemolytic anemia.
Question 6: A male patient with purple striae, thin skin, non-healing wound, and pedunculated abdomen, most probable cause?
- A. Insulin resistance
- B. Hypercortisolism (Correct Answer)
- C. Hypothyroidism
- D. Genetic connective tissue disorder
Explanation: Hypercortisolism - **Purple striae** are characteristic due to the breakdown of collagen and elastic fibers from excessive **cortisol**. - **Thin skin**, **non-healing wounds**, and a **pedunculated abdomen** (central obesity) are all classic signs of chronic high cortisol levels, as seen in **Cushing's syndrome** [1]. *Insulin resistance* - While insulin resistance can lead to conditions like **acanthosis nigricans** and **obesity**, it typically does not cause purple striae or thin skin directly. - It's often associated with **type 2 diabetes**, polycystic ovary syndrome, but not the specific dermatological features presented. *Hypothyroidism* - Hypothyroidism symptoms include **dry skin**, **coarse hair**, **fatigue**, and **weight gain**, but not typically purple striae or thin skin. - It can cause **non-pitting edema** (myxedema), which is distinct from the described skin changes. *Genetic connective tissue disorder* - Genetic connective tissue disorders like **Ehlers-Danlos syndrome** can cause thin, fragile skin and poor wound healing. - However, they do not typically present with the characteristic **purple striae** or **pedunculated abdomen** that point specifically to hypercortisolism.
Question 7: A 20-year-old chronic alcoholic presents with severe hematemesis. USG shows distension of portal vein and the liver appears hyperechoic. Pantoprazole has been initiated. What is the next step in management?
- A. Administer IV fluids and electrolytes to stabilize hemodynamics
- B. Perform an endoscopy to identify and treat varices (Correct Answer)
- C. Order a liver biopsy to assess for fibrosis
- D. Initiate a course of broad-spectrum antibiotics
Explanation: **Perform an endoscopy to identify and treat varices** - Severe **hematemesis** in a chronic alcoholic with signs of **portal hypertension** (distended portal vein, hyperechoic liver) strongly suggests bleeding esophageal varices [1]. - **Endoscopy** is crucial for both diagnosing the source of bleeding and providing immediate therapeutic intervention, such as **variceal band ligation** or **sclerotherapy** [1]. *Administer IV fluids and electrolytes to stabilize hemodynamics* - While **hemodynamic stabilization with IV fluids** is an immediate and critical step in managing severe GI bleeding, it is not the *next step in definitive management* after pantoprazole initiation, which aims to address the *cause* of the bleeding. - This is an initial supportive measure, but addressing the source of hemorrhage is paramount once stabilization begins [1]. *Order a liver biopsy to assess for fibrosis* - A **liver biopsy** is primarily used for diagnosing the underlying cause and severity of liver disease, such as **cirrhosis** and **fibrosis**. - It is not an urgent procedure in the context of acute, severe hematemesis and would delay critical interventions to stop the bleeding. *Initiate a course of broad-spectrum antibiotics* - **Antibiotics** are indeed utilized in patients with cirrhosis and upper GI bleeding to prevent **spontaneous bacterial peritonitis** and other infections, often administered *after* hemodynamic stabilization and initial endoscopic management. - However, stopping the active bleeding is the immediate priority before initiating prophylactic antibiotics.
Question 8: Which of the following statements about atrial fibrillation is correct?
- A. Rarely seen in heart with normal morphology
- B. Discrepancy in pulse rate and heart rate are reliable for diagnosis (Correct Answer)
- C. Cardioversion is used for all cases of atrial fibrillation
- D. Only digoxin used for rate control
Explanation: ***Discrepancy in pulse rate and heart rate are reliable for diagnosis*** - A disparity between the **apical heart rate** (auscultated at the chest) and the **peripheral pulse rate** (palpated at the wrist), known as a **pulse deficit**, is a characteristic sign of **atrial fibrillation**. [1] - This occurs because some ventricular contractions during atrial fibrillation are too weak to produce a palpable peripheral pulse, especially with a rapid, irregular ventricular response. [1] *Rarely seen in heart with normal morphology* - While atrial fibrillation is often associated with structural heart disease, it can occur in individuals without identifiable cardiac abnormalities, known as **lone atrial fibrillation**, especially in younger patients. [1] - Factors like **hypertension**, obesity, and sleep apnea can precipitate atrial fibrillation even in seemingly normal hearts. *Cardioversion is used for all cases of atrial fibrillation* - **Cardioversion** (electrical or pharmacological) is primarily used for **hemodynamically unstable** patients or stable patients for whom a **rhythm control strategy** is desired. [1] - Many patients, particularly those who are asymptomatic or have chronic atrial fibrillation, are managed with a **rate control strategy** and anticoagulation rather than cardioversion. [1] *Only digoxin used for rate control* - While **digoxin** can be used for **rate control** in atrial fibrillation, particularly in patients with heart failure or sedentary lifestyles, it is not the only agent. - **Beta-blockers** (e.g., metoprolol, atenolol) and **calcium channel blockers** (e.g., diltiazem, verapamil) are also commonly used as first-line agents for rate control in atrial fibrillation, especially if the patient tolerates them. [1]
Question 9: A patient presents with the following arterial blood gas (ABG) and electrolyte values: pH: 7.34, Na: 135 mEq/L, Cl: 93 mEq/L, HCO3: 20 mEq/L, Random Blood Sugar (RBS): 420 mg/dl. What is the most likely acid-base disturbance?
- A. Normal Anion Gap Metabolic Acidosis (NAGMA)
- B. Respiratory Acidosis
- C. High Anion Gap Metabolic Acidosis (HAGMA) (Correct Answer)
- D. Metabolic Alkalosis
Explanation: ### High Anion Gap Metabolic Acidosis (HAGMA) - The **pH (7.34)** indicates **acidemia**, and the **low bicarbonate (20 mEq/L)** suggests a metabolic acidosis [1], [2]. - Calculation of the anion gap: Na - (Cl + HCO3) = 135 - (93 + 20) = 22 mEq/L. An anion gap > 12 mEq/L is considered high, confirming **High Anion Gap Metabolic Acidosis (HAGMA)** [4]. The **RBS of 420 mg/dl** also points towards a likely cause such as **diabetic ketoacidosis** [3]. *Normal Anion Gap Metabolic Acidosis (NAGMA)* - This would be present if the calculated anion gap were within the normal range (typically 8-12 mEq/L). - Causes of NAGMA (e.g., hyperchloremic acidosis) are typically associated with increased chloride levels to compensate for the bicarbonate loss, which is not the primary finding here [4]. *Respiratory Acidosis* - This condition is characterized by a **low pH** and an **elevated PaCO2**, which is not provided but implied by the **low bicarbonate** not fitting a respiratory picture [2]. - While the pH is low, the primary disturbance given the other values (especially the low bicarbonate) is metabolic, not respiratory. *Metabolic Alkalosis* - Metabolic alkalosis is characterized by an **elevated pH** and an **elevated bicarbonate level**, which contradicts the presented values of low pH and low bicarbonate [2]. - This condition would involve a net gain of bicarbonate or a loss of acids, which is the opposite of the findings in this patient.
Question 10: Which of the following is not a complication of hypokalemia?
- A. Quadriparesis
- B. Cerebral edema (Correct Answer)
- C. Ventricular Tachycardia
- D. Diabetes insipidus
Explanation: ***Cerebral edema*** - **Cerebral edema** is typically associated with **hyponatremia** (low sodium levels), which causes hypotonicity in the extracellular fluid leading to water shifting into brain cells. - Hypokalemia primarily impacts neuromuscular and cardiac function and does not directly cause brain swelling due to fluid shifts. *Quadriparesis* - **Severe hypokalemia** can lead to **muscle weakness**, which can progress to flaccid paralysis affecting all four limbs (quadriparesis). - This occurs due to alterations in the **resting membrane potential** of muscle cells, making them less excitable. *Ventricular Tachycardia* - Hypokalemia can cause **cardiac arrhythmias**, including **ventricular tachycardia** and **fibrillation**, by prolonging repolarization and increasing myocardial excitability. - It can also lead to characteristic electrocardiogram (ECG) changes such as **flattened T waves**, **ST segment depression**, and prominent **U waves**. *Diabetes insipidus* - **Nephrogenic diabetes insipidus** can be a complication of chronic hypokalemia, where the kidneys become resistant to the effects of **antidiuretic hormone (ADH)**. - This results in the inability to concentrate urine, leading to **polyuria** (excessive urination) and **polydipsia** (excessive thirst).