Anatomy
1 questionsIn pediatric assessment, a cephalic index of 75-80 is classified as:
FMGE 2017 - Anatomy FMGE Practice Questions and MCQs
Question 71: In pediatric assessment, a cephalic index of 75-80 is classified as:
- A. Mesocephalic head shape (Correct Answer)
- B. Dolichocephalic head shape
- C. Brachycephalic head shape
- D. Scaphocephalic head shape
Explanation: ***Mesocephalic head shape*** - A cephalic index between **75 and 80** indicates a **mesocephalic** head shape, which means the head has a medium or normal width-to-length ratio. - This is considered the **average** or typical head shape in most populations. *Dolichocephalic head shape* - A **dolichocephalic** head shape is characterized by a cephalic index typically **below 75**, meaning the head is relatively **long and narrow**. - This head shape is often seen in individuals with certain genetic backgrounds or conditions that affect skull development. *Brachycephalic head shape* - A **brachycephalic** head shape is characterized by a cephalic index typically **above 80**, meaning the head is relatively **short and wide**. - This can be naturally occurring or a result of conditions like **craniosynostosis** [1] or positional molding. *Scaphocephalic head shape* - **Scaphocephaly** is a specific type of **dolichocephaly** resulting from the premature fusion of the **sagittal suture** [1]. - This condition leads to a very long, narrow, and keeled head shape that would fall into the severe dolichocephalic range (cephalic index well below 75).
Ophthalmology
1 questionsAll of the following are false about eye lid signs in GRAVES DISEASE except?
FMGE 2017 - Ophthalmology FMGE Practice Questions and MCQs
Question 71: All of the following are false about eye lid signs in GRAVES DISEASE except?
- A. Stellwag's sign: Incomplete and infrequent blinking (Correct Answer)
- B. Mobius sign: convergence insufficiency
- C. Dalrymple sign: lid retraction
- D. Von Graefe's sign: lid lag on downgaze
Explanation: **⚠️ QUESTION ISSUE: All four options are TRUE statements about Graves' disease, making this question technically flawed.** ***Stellwag's sign: Incomplete and infrequent blinking*** ✓ - **Stellwag's sign** is correctly defined as **incomplete and infrequent blinking**, causing a characteristic staring appearance. - This is a **TRUE** sign of **Graves' ophthalmopathy** due to sympathetic overactivity. - **Marked as correct answer**, but all options are actually true. *Mobius sign: convergence insufficiency* ✓ - **Moebius sign** is correctly defined as **convergence insufficiency** (inability to converge eyes for near vision). - This is a **TRUE** sign of **Graves' disease**. - Statement is medically accurate. *Dalrymple sign: lid retraction* ✓ - **Dalrymple's sign** is correctly defined as **lid retraction** (upper eyelid retraction exposing sclera above iris). - This is a **TRUE** and classic sign of **Graves' ophthalmopathy**. - Statement is medically accurate. *Von Graefe's sign: lid lag on downgaze* ✓ - **Von Graefe's sign** is correctly defined as **lid lag on downgaze** (upper eyelid lags behind eyeball during downward gaze). - This is a **TRUE** sign of **Graves' disease**. - Statement is medically accurate. **Educational Note:** This FMGE-2017 question is problematic because all four eyelid sign descriptions are medically accurate. In the actual exam, Stellwag's sign was likely considered the "best" answer, possibly because it's the most specific or commonly tested.
Orthopaedics
1 questionsA patient received an electric shock and fell down. He cannot do external rotation of shoulder and cannot move arm. What is the diagnosis:-
FMGE 2017 - Orthopaedics FMGE Practice Questions and MCQs
Question 71: A patient received an electric shock and fell down. He cannot do external rotation of shoulder and cannot move arm. What is the diagnosis:-
- A. Clavicle fracture
- B. Luxation erecta
- C. Posterior dislocation (Correct Answer)
- D. Anterior dislocation
Explanation: ***Posterior dislocation*** - An **electric shock** or **seizure** can cause strong muscle contractions, leading to a posterior shoulder dislocation. - Inability to perform **external rotation** and limited arm movement are classic signs of a posterior shoulder dislocation. *Clavicle fracture* - While a fall can cause a **clavicle fracture**, the primary symptoms would be pain over the clavicle and a visible deformity, not specifically limited external rotation or global arm immobility. - A clavicle fracture typically doesn't present with the specific inability to externally rotate the arm. *Luxation erecta* - **Luxatio erecta** is an inferior shoulder dislocation where the arm is held in an abducted and externally rotated position, pointing upwards, which is contrary to the described symptoms of inability to move the arm and external rotation. - It is a specific type of dislocation with a distinct presentation. *Anterior dislocation* - An **anterior dislocation** is the most common type of shoulder dislocation, but it usually presents with the arm held in slight abduction and external rotation, not an inability to externally rotate. - Typically results in a visible flattening of the deltoid contour and a prominent humeral head anteriorly.
Physiology
3 questionsThe PR interval in ECG denotes?
Which of these is true about SGLT1?
In the process shown below stretch stimulus is mediated by which of the following receptors?
FMGE 2017 - Physiology FMGE Practice Questions and MCQs
Question 71: The PR interval in ECG denotes?
- A. Ventricular depolarization and ventricular repolarization
- B. Atrial depolarization with atrial repolarization
- C. Atrial depolarization with A - V conduction (Correct Answer)
- D. Atrial depolarization only
Explanation: ***Atrial depolarization with A - V conduction*** * The **PR interval** reflects the time from the beginning of **atrial depolarization** (P wave) to the beginning of **ventricular depolarization** (QRS complex). * It represents the time taken for the electrical impulse to travel through the **atria** and the **AV node** to the ventricles. *Ventricular depolarization and ventricular repolarization* * **Ventricular depolarization** is represented by the **QRS complex**, and **ventricular repolarization** is represented by the **T wave**. * The PR interval occurs before the QRS complex, not during ventricular depolarization or repolarization. *Atrial depolarization with atrial repolarization* * **Atrial depolarization** is represented by the **P wave**. * **Atrial repolarization** typically occurs simultaneously with **ventricular depolarization** (QRS complex) and is often obscured by it. The PR interval includes the P wave but extends beyond it. *Atrial depolarization only* * **Atrial depolarization** is solely represented by the **P wave**. * The PR interval is a longer duration that includes the P wave and the subsequent delay in the **AV node**.
Question 72: Which of these is true about SGLT1?
- A. Secondary active transport of glucose in prostate
- B. Secondary active transport of glucose in brain
- C. Secondary active transport of glucose in intestine (Correct Answer)
- D. Secondary active transport of glucose in rods and cones
Explanation: ***Secondary active transport of glucose in intestine*** - **SGLT1** is the primary transporter responsible for **glucose and galactose absorption** from the lumen of the small intestine into the enterocytes. - It uses the electrochemical gradient of **sodium** to co-transport glucose against its concentration gradient, classifying it as **secondary active transport**. *Secondary active transport of glucose in prostate* - While glucose is vital for prostate metabolism, its transport predominantly involves **GLUTs** (e.g., GLUT1), not SGLT1. - SGLT1 is generally not found in significant amounts in the prostate. *Secondary active transport of glucose in brain* - Glucose transport across the **blood-brain barrier** and into brain cells is primarily mediated by **GLUT1** and other GLUT transporters, which are **facilitated diffusers**, not SGLT1. - SGLT1 has a very limited role, if any, in normal brain glucose uptake. *Secondary active transport of glucose in rods and cones* - Retinal photoreceptors (rods and cones) indeed rely on glucose, but its uptake is mainly via **GLUT1** and other GLUT family members. - **SGLT1** is not a significant transporter for glucose in these cells.
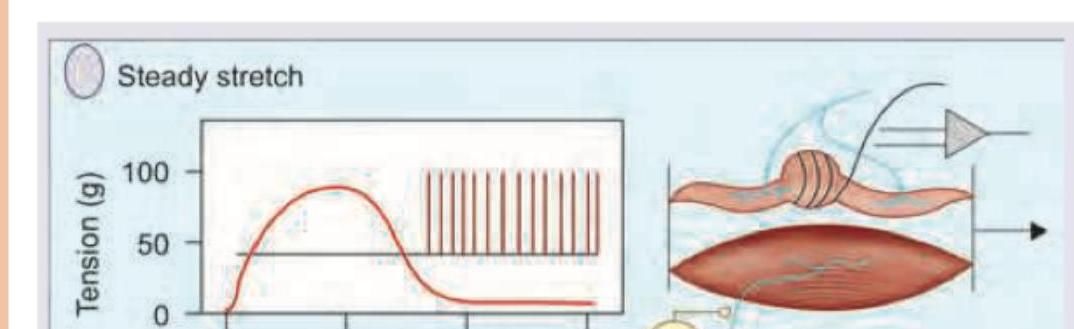
Question 73: In the process shown below stretch stimulus is mediated by which of the following receptors?
- A. Merkel's disc
- B. Meissner's corpuscle
- C. Pacinian corpuscle
- D. Muscle spindle (Correct Answer)
Explanation: ***Muscle spindle*** - The image depicts a **muscle**, and the "Steady stretch" stimulus clearly shows an increase in muscle tension followed by sustained neural firing, characteristic of a **stretch reflex**. - **Muscle spindles** are proprioceptors located within skeletal muscles that detect changes in muscle length and the rate of change of length, playing a crucial role in the stretch reflex. *Merkel's disc* - **Merkel's discs** are mechanoreceptors located in the basal layer of the epidermis, primarily responsible for detecting sustained light touch and pressure. - They are not involved in sensing muscle stretch. *Meissner's corpuscle* - **Meissner's corpuscles** are rapidly adapting mechanoreceptors found in the dermal papillae, specialized for detecting light touch and low-frequency vibration. - They are cutaneous receptors and do not mediate muscle stretch. *Pacinian corpuscle* - **Pacinian corpuscles** are rapidly adapting mechanoreceptors located deep in the dermis and subcutaneous tissue, sensitive to deep pressure and high-frequency vibration. - They are not responsible for detecting muscle stretch.
Psychiatry
2 questionsWhich of the following terms describes sexual attraction or relationships primarily between women?
Indoor management of anorexia nervosa is done on priority patients with:-
FMGE 2017 - Psychiatry FMGE Practice Questions and MCQs
Question 71: Which of the following terms describes sexual attraction or relationships primarily between women?
- A. Masochism
- B. Nymphomania
- C. Transsexualism
- D. Lesbianism (Correct Answer)
Explanation: ***Lesbianism*** - **Lesbianism** describes sexual attraction or relationships primarily between **women**. - It is a form of **homosexuality**, specifically referring to female same-sex attraction. *Masochism* - **Masochism** is a paraphilia where sexual gratification is derived from experiencing **pain, humiliation, or bondage**. - This term does not describe the gender of individuals involved in a sexual relationship. *Nymphomania* - **Nymphomania** is an outdated and stigmatizing term historically used to describe a woman with an **uncontrollably strong desire for sexual activity**. - It does not refer to the gender of the individuals involved in the sexual attraction. *Transsexualism* - **Transsexualism** refers to the condition of a **transgender person** who identifies with a sex different from their birth sex and often seeks to transition through medical interventions. - This term describes **gender identity** rather than sexual orientation or the gender composition of a relationship.
Question 72: Indoor management of anorexia nervosa is done on priority patients with:-
- A. Depression
- B. Amenorrhea
- C. Binging episodes
- D. Weight for height less than 75% of normal (Correct Answer)
Explanation: ***Weight for height less than 75% of normal*** - A **weight for height less than 75% of normal** (or **BMI <15 kg/m²**) indicates severe **malnutrition** and a high risk of medical complications, necessitating urgent inpatient care. - This level of **underweight** is a critical indicator for hospital admission in **anorexia nervosa** to prevent severe organ dysfunction, refeeding syndrome, and even death. *Depression* - While **depression** is a common comorbidity with **anorexia nervosa** and often requires treatment, it does not, by itself, warrant immediate inpatient management unless there are acute **suicidal risks**. - **Depression** is usually managed in an outpatient setting initially, with hospitalization being reserved for severe cases where safety is compromised. *Amenorrhea* - **Amenorrhea** (absence of menstruation) is a common symptom of **anorexia nervosa** due to hormonal imbalances caused by low body weight. - Though an indicator of significant caloric restriction, **amenorrhea** alone is not typically an immediate criterion for inpatient admission unless accompanied by other severe physical complications. *Binging episodes* - While **binging episodes** can occur in **anorexia nervosa** (specifically the binge-purging subtype) and can lead to electrolyte imbalances or medical complications, they are not the primary, stand-alone trigger for immediate inpatient admission. - The severity of **binging** and associated **purging behaviors** must be evaluated in the context of overall medical stability and weight to determine the appropriate level of care.