
Neurology

On this page
Recognising Acute Neurological Presentations
A 68-year-old woman arrives at 08:30 with right-sided weakness and speech difficulty that began at breakfast. Her husband notes symptom onset was 45 minutes ago. This scenario demands immediate stroke pathway activation-every 15-minute delay to thrombolysis costs an average of one month of disability-free life. Recognising acute neurological emergencies and distinguishing them from mimics requires systematic assessment, precise timing documentation, and rapid decision-making that directly impacts patient outcomes.
-
Stroke recognition tools:
- FAST (Face-Arm-Speech-Time): 89% sensitivity, 90% specificity for stroke
- ROSIER score >0 indicates stroke (sensitivity 92%, specificity 86%)
- Posterior circulation strokes often missed: isolated vertigo, diplopia, ataxia
- Time of symptom onset (or last known well) is the single most critical data point
-
Seizure identification :
- Generalised tonic-clonic: loss of consciousness, rhythmic jerking, post-ictal confusion lasting 15-30 minutes
- Focal seizures: preserved awareness possible, automatisms, Todd's paresis (transient weakness post-seizure mimicking stroke)
- Status epilepticus definition: >5 minutes continuous seizure activity or recurrent seizures without recovery
- First seizure requires 12-lead ECG (exclude long QT), glucose, electrolytes, neuroimaging within 24 hours (NICE CG150)
| Presentation | Key Discriminator | Time-Critical Action |
|---|---|---|
| Acute stroke | Sudden onset, maximal deficit at onset | CT head within 1 hour of arrival |
| TIA | Symptoms resolved, typically <1 hour | ABCD² score, specialist assessment within 24h if score ≥4 |
| Seizure | Witnessed ictal activity, post-ictal phase | Protect airway, time seizure, IV access |
| Syncope | Prodrome, rapid recovery, no focal signs | ECG, postural BP, consider cardiac cause |
🚩 Red Flag: Sudden-onset "worst headache of life" is subarachnoid haemorrhage until proven otherwise-CT head has 98% sensitivity within 6 hours, declining to 50% by 1 week.
Recognising Acute Neurological Presentations


Understanding Pathophysiological Mechanisms
Ischaemic stroke pathophysiology centres on the ischaemic penumbra-tissue surrounding the infarct core that remains viable for 4.5-6 hours through collateral circulation. This penumbra represents salvageable brain: each minute of untreated large vessel occlusion destroys 1.9 million neurons. Thrombolysis and thrombectomy target penumbral rescue, explaining strict time windows. Haemorrhagic transformation risk increases with larger infarcts, delayed reperfusion, and anticoagulation, occurring in 15% of ischaemic strokes.
-
Stroke mechanisms:
- Large artery atherosclerosis (35%): carotid stenosis >50% increases stroke risk 2-3 fold
- Cardioembolic (25%): AF increases stroke risk 5-fold, warfarin reduces this by 64%
- Small vessel disease (25%): lacunar infarcts <15mm, associated with hypertension and diabetes
- Cryptogenic (15%): prolonged cardiac monitoring detects paroxysmal AF in 16% within 30 days
-
Dementia and delirium pathways :
- Alzheimer's: amyloid-β plaques and tau tangles cause synaptic dysfunction and neuronal death
- Vascular dementia: stepwise decline, white matter hyperintensities, subcortical ischaemia
- Delirium: multifactorial-infection, drugs, metabolic disturbance cause neurotransmitter imbalance (acetylcholine deficiency, dopamine excess)
- Delirium increases dementia risk 8-fold and mortality 2-fold at 1 year
-
Migraine mechanisms :
- Cortical spreading depression: wave of neuronal depolarisation propagates at 3mm/min across cortex
- Trigeminovascular activation: calcitonin gene-related peptide (CGRP) release causes meningeal inflammation and pain
- Aura symptoms reflect cortical spreading depression: visual (90%), sensory (30%), speech (10%)
Understanding Pathophysiological Mechanisms


Applying Investigations and Scoring Systems
A 72-year-old man presents with transient right arm weakness lasting 20 minutes, now resolved. ABCD² score calculation: Age ≥60 (1 point), BP 165/95 (1 point), unilateral weakness (2 points), duration 10-59 minutes (1 point), no diabetes = 5 points. NICE NG128 mandates specialist assessment and imaging within 24 hours for scores ≥4, as 7-day stroke risk is 11.7% versus 0.4% for score 0-3.
-
Stroke imaging :
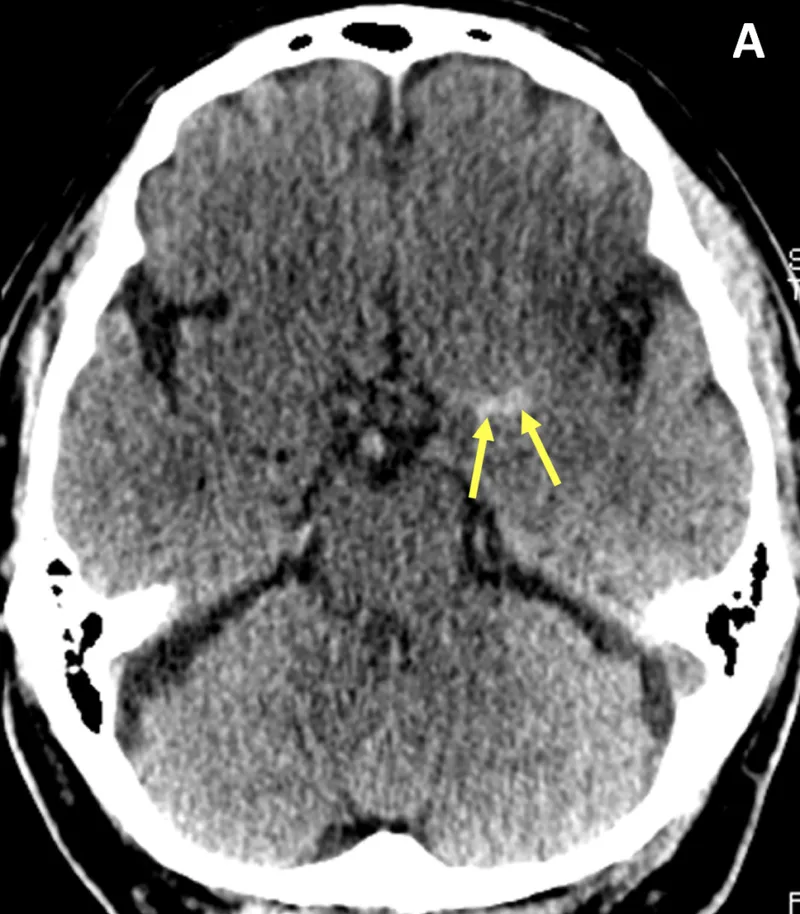
- Non-contrast CT: 95% sensitivity for haemorrhage, early ischaemic signs (insular ribbon loss, hyperdense vessel sign) present in 60% within 3 hours
- CT angiography: identifies large vessel occlusion for thrombectomy consideration (up to 24 hours with perfusion mismatch)
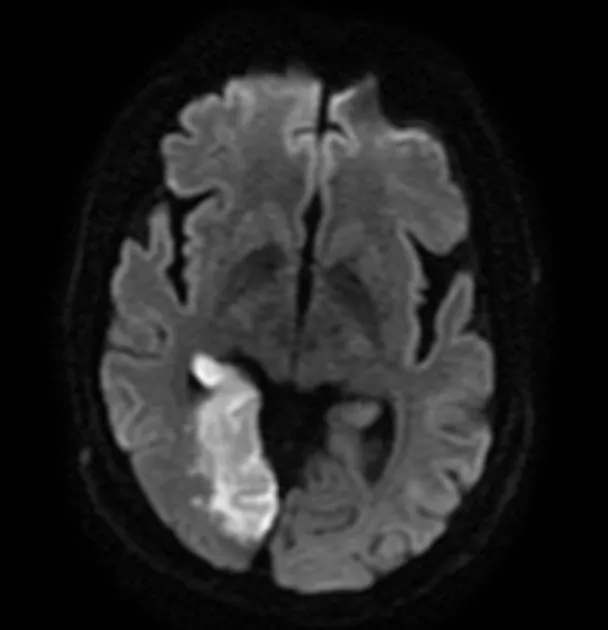
- MRI diffusion-weighted imaging: 88-100% sensitivity for acute infarction within 3 hours, superior for posterior circulation
-
Seizure investigations :
- EEG within 24 hours if diagnostic uncertainty or suspected non-convulsive status
- MRI brain (not CT) for first seizure: identifies structural lesion in 10-15%
- Prolactin: rises 2-3 fold within 20 minutes of generalised tonic-clonic seizure, returns to baseline by 60 minutes
-
Delirium assessment :
- 4AT score: ≥4 indicates possible delirium/cognitive impairment (sensitivity 89%, specificity 84%)
- Identify precipitant: infection (40%), drugs (30%), metabolic (15%), intracranial (5%)
- Confusion screen: FBC, U&E, calcium, glucose, LFT, TFT, B12, urinalysis, CXR, ECG
| Investigation | Indication | Diagnostic Yield |
|---|---|---|
| CT head non-contrast | All suspected strokes within 1h | Haemorrhage 95%, early ischaemia 60% |
| MRI brain with DWI | First seizure, diagnostic uncertainty | Structural lesion 10-15% |
| Carotid Doppler ultrasound | Anterior circulation TIA/stroke | Significant stenosis 15-20% |
| 12-lead ECG | All stroke/TIA patients | Atrial fibrillation 10-15% |
Applying Investigations and Scoring Systems
Analysing Differential Diagnoses
Stroke mimics account for 30% of suspected strokes presenting to hyperacute units. Seizures with Todd's paresis cause transient focal weakness lasting minutes to hours, but seizure history or witnessed ictal activity provides the key discriminator. Hypoglycaemia (<3.0 mmol/L) causes focal neurology in 15% of cases-immediate glucose measurement is mandatory. Functional neurological disorder presents with non-anatomical deficits, inconsistent examination findings, and often positive Hoover's sign.
-
Headache differentials :
- Migraine with aura: gradual symptom onset over 5-20 minutes, positive visual phenomena (zigzags), headache follows aura
- TIA: sudden onset, negative symptoms (vision loss, not scintillations), no headache
- Subarachnoid haemorrhage: thunderclap onset (<1 minute to peak), neck stiffness, photophobia
- Giant cell arteritis (>50 years): jaw claudication, scalp tenderness, ESR >50 mm/h
-
Delirium versus dementia :
- Delirium: acute onset (hours-days), fluctuating course, inattention prominent, reversible in 60%
- Dementia: insidious onset (months-years), progressive decline, memory loss prominent, irreversible
- Delirium superimposed on dementia occurs in 50% of hospitalised dementia patients
| Feature | Stroke | Seizure with Todd's Paresis | Hypoglycaemia | Functional |
|---|---|---|---|---|
| Onset | Sudden, maximal at start | Post-ictal, gradual improvement | Variable, confusion prominent | Gradual, inconsistent |
| Consciousness | Often preserved | Impaired post-ictally | Often impaired | Preserved |
| Glucose | Normal | Normal | <3.0 mmol/L | Normal |
| Imaging | Acute infarct/haemorrhage | Normal (or old changes) | Normal | Normal |
Analysing Differential Diagnoses
Evaluating Evidence-Based Treatments
Alteplase 0.9 mg/kg (maximum 90mg) administered within 4.5 hours of ischaemic stroke onset reduces disability (NNT=10 for favourable outcome at 3 months) but increases symptomatic intracranial haemorrhage risk (4% versus 0.6% placebo). Contraindications include BP >185/110 mmHg despite treatment, previous intracranial haemorrhage, recent surgery/trauma within 2 weeks, and anticoagulation with INR >1.7. Mechanical thrombectomy for large vessel occlusion extends the window to 24 hours when perfusion imaging demonstrates salvageable tissue.
-
Acute seizure management :
- First-line: IV lorazepam 4mg or buccal midazolam 10mg (5-10 minutes)
- Second-line (if seizure continues): IV levetiracetam 40 mg/kg (max 3g) or phenytoin 20 mg/kg at 50 mg/min
- Status epilepticus (>30 minutes): general anaesthesia with propofol/thiopental, ICU admission
- Long-term: start antiepileptic after second unprovoked seizure (reduces 2-year recurrence from 51% to 25%)
-
Migraine treatment :
- Acute: oral triptan (sumatriptan 50-100mg) plus NSAID within 1 hour of onset (NNT=3-4 for pain-free at 2 hours)
- Prophylaxis (≥4 attacks/month): propranolol 80-160mg daily (reduces attack frequency by 50% in 60% of patients)
- CGRP monoclonal antibodies: erenumab 70mg SC monthly for refractory cases (reduces monthly migraine days by 4-5)
- Avoid opioids and frequent triptans (>10 days/month) due to medication-overuse headache risk
| Drug | Indication | Dose | Key Monitoring |
|---|---|---|---|
| Alteplase | Ischaemic stroke <4.5h | 0.9 mg/kg IV (max 90mg) | Neuro obs every 15min for 2h, then hourly for 24h |
| Levetiracetam | Focal epilepsy | 500mg BD, increase to 1500mg BD | Mood changes, renal function |
| Sumatriptan | Acute migraine | 50-100mg PO (max 300mg/24h) | Cardiovascular disease contraindication |
| Donepezil | Alzheimer's dementia | 5mg daily, increase to 10mg after 4 weeks | Bradycardia, GI upset |
Evaluating Evidence-Based Treatments
Synthesising Complex Multidisciplinary Care
An 82-year-old woman with previous stroke, AF on apixaban, and moderate dementia presents with recurrent falls and confusion. Her ABCD² score is 6 following transient dysphasia. Management requires balancing stroke prevention (continue anticoagulation despite fall risk-absolute stroke reduction 2.7%/year outweighs bleeding risk 1.3%/year) with delirium management (identify precipitant, avoid antipsychotics if possible due to stroke risk) and stroke secondary prevention optimisation.
-
Post-stroke care :
- Antiplatelet: clopidogrel 75mg daily (or aspirin 75mg plus dipyridamole MR 200mg BD)
- Anticoagulation for AF: DOAC preferred (apixaban 5mg BD, rivaroxaban 20mg daily, edoxaban 60mg daily)
- Statin: atorvastatin 80mg regardless of baseline cholesterol
- BP target <130/80 mmHg after 2 weeks (avoid lowering acutely unless >220/120 mmHg)
- Early supported discharge: reduces length of stay by 7 days, improves independence (OR 1.6)
-
Dementia multidisciplinary input:
- Cognitive assessment: Montreal Cognitive Assessment (MoCA) score <26 indicates impairment
- Capacity assessment for treatment decisions, advance care planning
- Occupational therapy: home safety assessment, falls prevention strategies
- Carer support: respite care, lasting power of attorney, benefits advice
| Comorbidity | Management Consideration | Evidence-Based Approach |
|---|---|---|
| AF + dementia | Anticoagulation despite fall risk | Continue DOAC unless fall frequency >295/year |
| Stroke + diabetes | Glucose control | Target HbA1c <53 mmol/mol, avoid hypoglycaemia |
| Epilepsy + pregnancy | Teratogenicity risk | Levetiracetam or lamotrigine monotherapy, high-dose folic acid 5mg |
| Migraine + cardiovascular disease | Triptan contraindication | Avoid triptans, use NSAIDs or neuromodulation |
Synthesising Complex Multidisciplinary Care
High Yield Summary
Key Take-Aways:
- Stroke thrombolysis within 4.5 hours: alteplase 0.9 mg/kg (max 90mg) reduces disability, NNT=10
- ABCD² score ≥4 mandates specialist assessment within 24 hours (7-day stroke risk 11.7%)
- Status epilepticus: IV lorazepam 4mg first-line, second-line levetiracetam 40 mg/kg or phenytoin 20 mg/kg
- Migraine acute treatment: triptan plus NSAID within 1 hour (NNT=3-4 for pain-free at 2 hours)
- Delirium 4AT score ≥4 indicates cognitive impairment; identify and treat precipitant
- CT head within 1 hour for suspected stroke; MRI brain for first seizure
- Anticoagulation for AF reduces stroke by 64%; continue despite fall risk unless >295 falls/year
Essential Neurology Numbers:
| Parameter | Critical Value | Clinical Significance |
|---|---|---|
| Stroke thrombolysis window | <4.5 hours | Each 15-min delay costs 1 month disability-free life |
| ABCD² high risk | ≥4 points | 7-day stroke risk 11.7% |
| Status epilepticus definition | >5 minutes | Requires immediate benzodiazepine treatment |
| Hypoglycaemia threshold | <3.0 mmol/L | Can mimic stroke in 15% of cases |
| CT sensitivity for SAH | 98% at 6h, 50% at 7 days | LP required if CT negative and high suspicion |
Key Principles:
- Time is brain: 1.9 million neurons die per minute in large vessel occlusion
- Stroke mimics (30% of presentations): hypoglycaemia, seizure, functional-always check glucose
- Anticoagulation benefits outweigh bleeding risk in AF unless extreme fall frequency
- Delirium is multifactorial and reversible in 60%-systematic precipitant identification essential
- Avoid medication-overuse headache: limit acute migraine treatment to <10 days/month
Quick Reference:
| Condition | First Investigation | First Treatment | Time-Critical Action |
|---|---|---|---|
| Suspected stroke | CT head within 1h | Alteplase if <4.5h | Door-to-needle <60 min |
| Seizure >5 min | IV access, glucose | Lorazepam 4mg IV | Protect airway, time seizure |
| TIA (ABCD² ≥4) | Carotid Doppler, echo | Aspirin 300mg stat | Specialist review <24h |
| Acute migraine | Clinical diagnosis | Triptan + NSAID | Treat within 1h of onset |
Continue reading on Oncourse
Sign up for free to access the full lesson, plus unlimited questions, flashcards, AI-powered notes, and more.
CONTINUE READING — FREEor get the app
Have doubts about this lesson?
Ask Rezzy, your AI Study Mate, to explain anything you didn't understand
Practice Questions: Neurology
Test your understanding with these related questions
A 42-year-old woman presents with fatigue, muscle aches, and widespread pain. She has multiple tender points but normal inflammatory markers. Sleep is poor. What is the most appropriate initial treatment?