

Quick Overview
Dementia and delirium represent distinct but clinically overlapping cognitive syndromes requiring urgent differentiation. Delirium is an acute, fluctuating confusional state (medical emergency), while dementia is a chronic, progressive decline. The 4AT score enables rapid bedside differentiation, and NICE NG97 provides structured guidance on investigation, diagnosis, and pharmacological management of dementia subtypes.
Core Facts & Concepts
Delirium vs Dementia Key Features:
| Feature | Delirium | Dementia |
|---|---|---|
| Onset | Hours-days (acute) | Months-years (insidious) |
| Course | Fluctuating (worse at night) | Progressive, stable daily |
| Attention | Severely impaired | Preserved until late |
| Consciousness | Altered/clouded | Alert until advanced |
| Reversibility | Often reversible | Irreversible (mostly) |
4AT Score (Delirium Screening):
- 0 = Delirium unlikely
- 1-3 = Possible cognitive impairment
- ≥4 = Probable delirium
- Components: Alertness (0-4), AMT4 (0-2), Attention (0-2), Acute change (0-4)
Reversible Causes of Dementia (Screen All):
- Vitamin B12/folate deficiency (<200 ng/L)
- Hypothyroidism (TSH >10 mU/L)
- Hypercalcaemia (>2.6 mmol/L)
- Normal pressure hydrocephalus (triad: dementia, gait apraxia, incontinence)
- Chronic subdural haematoma
- Depression ("pseudodementia")
Cognitive Assessment Tools:
- ACE-III: 100-point scale (≥88 = normal, <82 = impaired)
- MoCA: 30-point scale (≥26 = normal, sensitive to mild cognitive impairment)
- MMSE: 30-point scale (outdated, copyright issues)
Problem-Solving Approach
Step 1: Exclude Delirium First
- Apply 4AT score at bedside (takes 2 minutes)
- If ≥4: Investigate for underlying cause (sepsis, drugs, metabolic, hypoxia)
- Manage delirium before assessing for dementia
Step 2: Confirm Dementia Diagnosis
- Cognitive impairment affecting ≥2 domains (memory, language, executive, visuospatial)
- Functional decline in ADLs
- Duration >6 months
- Not explained by delirium/psychiatric disorder
Step 3: Investigate Reversible Causes (NICE NG97)
- Bloods: FBC, U&E, LFTs, calcium, glucose, TSH, B12/folate
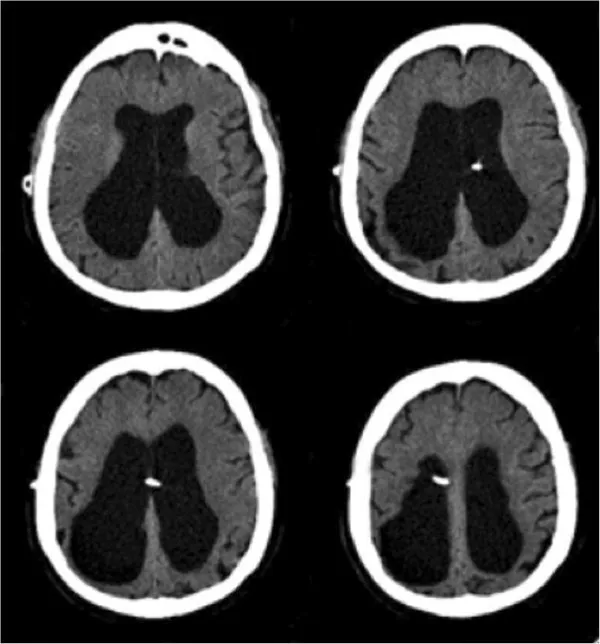
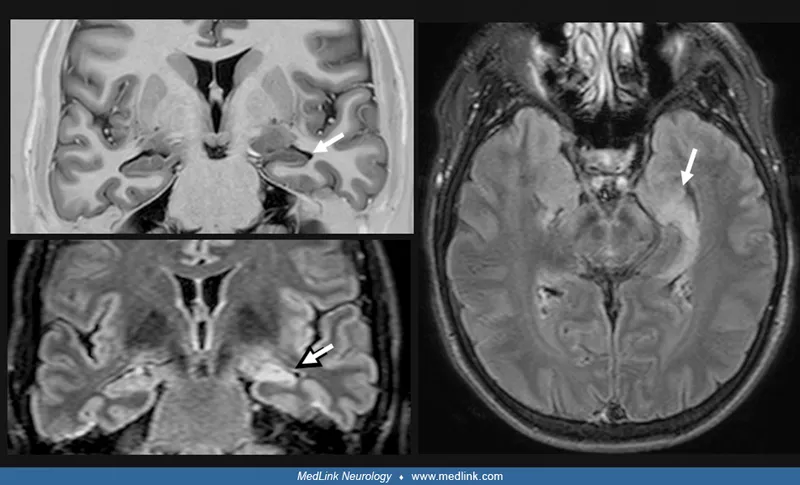
- Neuroimaging: MRI brain (or CT if contraindicated)
- Consider: HIV, syphilis serology if risk factors
Step 4: Subtype Classification
- Alzheimer's (60%): Gradual memory loss, temporal/hippocampal atrophy
- Vascular (20%): Stepwise decline, stroke history, white matter changes
- Lewy body (15%): Visual hallucinations, parkinsonism, fluctuating cognition
- Frontotemporal (5%): Personality change, disinhibition, frontal atrophy
🚩 Red Flags: Age <60, rapid progression (<2 years), focal neurology, headache, seizures → refer neurology urgently
Analysis Framework
Acetylcholinesterase Inhibitors (NICE NG97 Criteria):
| Drug | Dementia Type | Initiation Criteria | MMSE Range |
|---|---|---|---|
| Donepezil | Alzheimer's, Lewy body | Mild-moderate | 10-26 |
| Rivastigmine | Alzheimer's, Lewy body, Parkinson's | Mild-moderate | 10-26 |
| Galantamine | Alzheimer's only | Mild-moderate | 10-26 |
| Memantine | Moderate-severe Alzheimer's | MMSE <10 OR intolerant to above | <20 |
When to Start Treatment (All Required):
- Confirmed Alzheimer's/Lewy body dementia diagnosis
- MMSE 10-26 (mild-moderate)
- Specialist (memory clinic) initiation
- Review at 3 months (continue if MMSE stable/improved AND functional benefit)
⚠️ Warning: Do NOT use antipsychotics routinely in dementia (↑ stroke risk, ↑ mortality). Reserve for severe distress/risk only.
Visual Aid
Delirium Precipitants Mnemonic:
📌 Remember: PINCH ME - Pain, Infection, Nutrition, Constipation, Hydration, Medication, Environment
Key Points Summary
✓ 4AT score ≥4 = probable delirium (medical emergency requiring urgent investigation)
✓ Dementia diagnosis requires: ≥2 cognitive domains affected + functional decline + >6 months duration
✓ Always screen reversible causes: B12, folate, TSH, calcium + MRI brain (NICE NG97 mandatory)
✓ Acetylcholinesterase inhibitors (donepezil/rivastigmine/galantamine): Start if Alzheimer's/Lewy body + MMSE 10-26 + specialist initiation
✓ Memantine: Reserved for moderate-severe Alzheimer's (MMSE <20) or intolerance to cholinesterase inhibitors
✓ Avoid antipsychotics in dementia unless severe distress/risk (↑ stroke, ↑ mortality)
✓ ACE-III >88 = normal, <82 = cognitive impairment (more sensitive than MMSE for mild cases)
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more