

Melanocyte & Melanin - The Colour Code
- Melanocytes:
- Origin: Neural crest cells.
- Location: Epidermal basal layer (ratio ~1:10 keratinocytes), hair matrix, uvea, inner ear.
- Function: Synthesizes melanin within melanosomes.
- Melanin Synthesis:
- Key enzyme: Tyrosinase (copper-dependent).
- Pathway: $L-Tyrosine \xrightarrow{Tyrosinase} L-DOPA \xrightarrow{Tyrosinase} Dopaquinone \rightarrow Melanins$.
- Types: Eumelanin (brown/black), Pheomelanin (yellow/red, cysteine-rich).
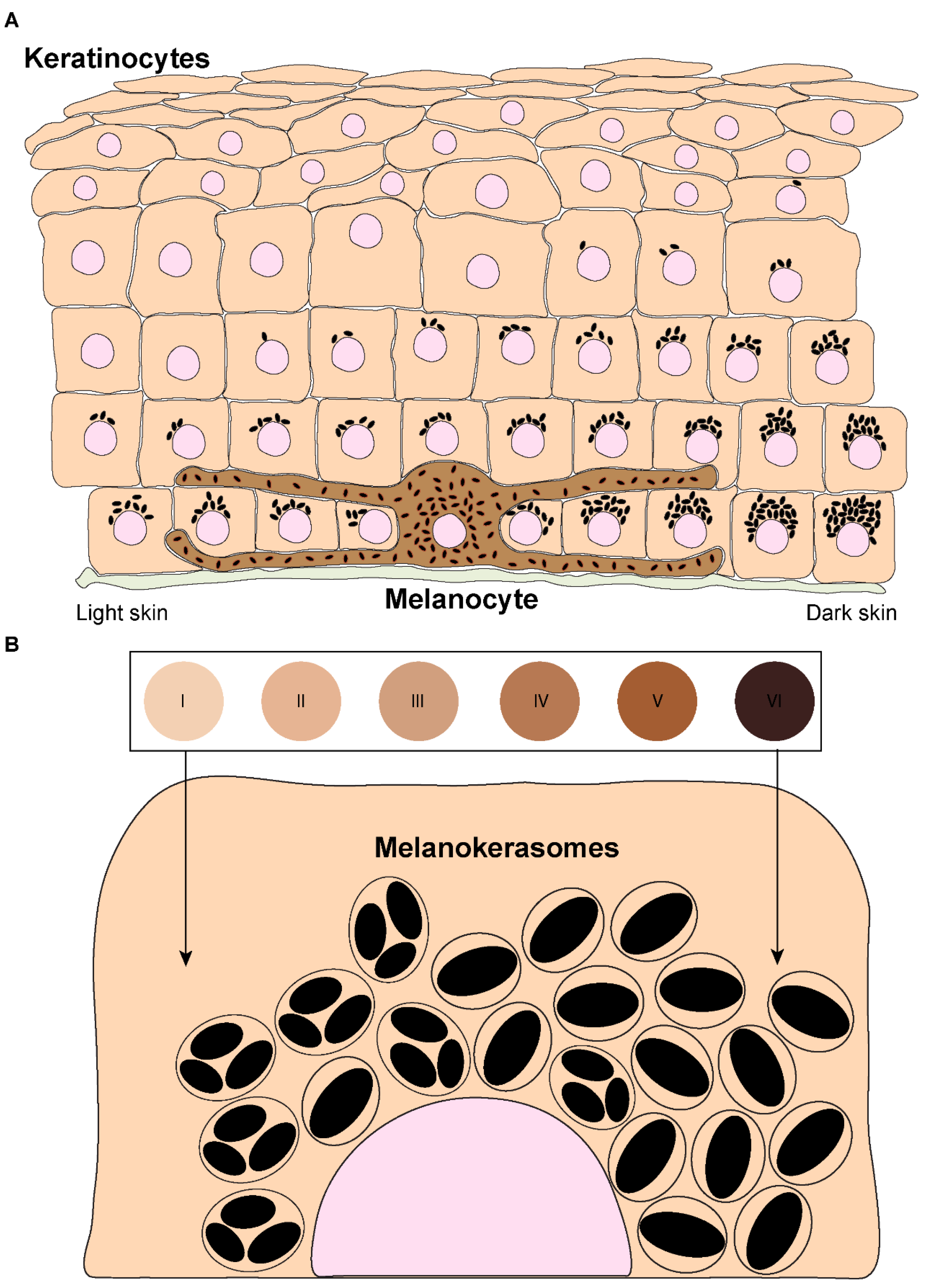
- Melanosomes: Lysosome-related organelles for melanin synthesis, storage, transfer to keratinocytes.
- Skin Color: Determined by melanocyte activity, melanosome type/size/distribution, degradation rate; not melanocyte number.
- Regulation: UV radiation, MSH, ACTH stimulate melanogenesis.
Loading diagram…
> ⭐ Oculocutaneous albinism Type 1 (OCA1): *TYR* gene mutations cause deficient tyrosinase activity, reducing melanin.
Hypopigmentation - When Colour Fades
| Feature | Vitiligo | Albinism (OCA) | Piebaldism |
|---|---|---|---|
| Etiology | Autoimmune melanocyte destruction; genetic factors | Genetic defect, melanin synthesis (TYR gene) | Autosomal dominant; KIT gene; melanoblast migration defect |
| Clinical | Acquired, progressive patches; Koebner +ve | Congenital hypopigmentation (skin, hair, eyes); nystagmus, photophobia | Congenital white forelock (poliosis); stable, symmetrical midline patches |
| Histology | Melanocytes absent; T-cell infiltrate | Melanocytes present; melanin ↓/absent | Melanocytes absent in depigmented areas |
| Key Dx | Wood's lamp (chalky white); autoimmune screen (thyroid) | Ocular signs (nystagmus); family Hx; genetic test | Stable since birth; characteristic distribution; family Hx +ve |
Hyperpigmentation - The Darker Side
- Increased melanin production or deposition.
| Feature | Melasma | Post-Inflammatory Hyperpigmentation (PIH) | Lentigines (Solar/Senile) | Ephelides (Freckles) |
|---|---|---|---|---|
| Etiology | Hormonal (pregnancy, OCPs), UV exposure | Post-inflammatory (acne, eczema) | Chronic UV exposure, aging | Genetic, UV exposure |
| Clinical | Symmetrical, irregular, brownish macules/patches on sun-exposed areas (face) | Macules/patches at site of prior inflammation | Well-demarcated, brown macules/patches on sun-exposed areas | Small, light brown macules, darken with sun |
| Histology | ↑ Melanin in epidermis ± dermis (melanophages); normal melanocyte count | ↑ Melanin in epidermis ± dermis (melanophages); variable melanocyte count | ↑ Melanin in basal layer, elongated rete ridges, normal/↑ melanocytes | ↑ Melanin in basal keratinocytes, normal melanocyte count |
⭐ Riehl's melanosis is a pigmented contact dermatitis, often seen on the face and neck, presenting as diffuse greyish-brown hyperpigmentation. It's a form of PIH.
- Wood's lamp: Epidermal melasma is accentuated; dermal is not. (📌 Epidermal Enhanced)
- Lentigo maligna: A melanoma in situ, presents as an enlarging, irregular pigmented macule on sun-damaged skin, especially in elderly individuals. Requires biopsy for diagnosis.
Nevi & Melanoma - Moles & Red Flags
Benign melanocytic nevi (moles) are common. Malignant melanoma is a deadly skin cancer; early detection is key.
| Nevus Type | Location | Key Features |
|---|---|---|
| Junctional | Epidermis | Flat, dark; nests at D-E jct. |
| Compound | Epidermis/Dermis | Raised, pigmented; nests epi & dermis |
| Intradermal | Dermis | Dome-shaped, flesh/light brown; older adults |
| Blue Nevus | Dermis | Blue-black; spindle cells, Tyndall effect |
| Spitz Nevus | Children (often) | Pink/red papule; histologically mimics melanoma |
📌 ABCDE Criteria for Melanoma Detection:
- Asymmetry: One half unlike the other.
- Border: Irregular, scalloped, or poorly defined.
- Color: Varied (shades of tan, brown, black; may include red, white, blue).
- Diameter: Usually > 6 mm (pencil eraser size).
- Evolving: Change in size, shape, color, elevation, or new symptom (e.g., bleeding, itching, crusting).
⭐ Acral lentiginous melanoma is the most common type in dark-skinned individuals, often found on palms, soles, or under nails (subungual).
High‑Yield Points - ⚡ Biggest Takeaways
- Vitiligo: Autoimmune melanocyte destruction causes depigmented patches; Koebner phenomenon often positive.
- Albinism: Genetic tyrosinase deficiency (e.g., OCA1) impairs melanin synthesis; normal melanocyte count.
- Melasma: Hormonally-influenced hyperpigmentation, typically on sun-exposed facial areas; exacerbated by UV.
- Acanthosis Nigricans: Velvety, hyperpigmented plaques in flexures; signals insulin resistance or internal malignancy.
- Lentigo Solaris: Benign "age spots" from chronic sun exposure; characterized by ↑ melanocyte number.
- Café-au-lait Macules: Multiple large macules are a diagnostic criterion for Neurofibromatosis Type 1 (NF1).
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more