

Pelvic Floor Anatomy and Function - The Body's Hammock

- Musculofascial sling supporting pelvic viscera; forms base of abdominopelvic cavity.
- Key Components:
- Pelvic Diaphragm (main support):
- Levator ani (puborectalis, pubococcygeus, iliococcygeus).
- Coccygeus muscles.
- Perineal Membrane & associated muscles: Urogenital support.
- Pelvic Diaphragm (main support):
- Innervation: Primarily Pudendal nerve (S2-S4); direct sacral nerve branches.
- Functions: Supports organs, maintains continence (urinary/fecal), sexual function, aids childbirth.
⭐ Damage to the levator ani or pudendal nerve during childbirth is a major risk factor for pelvic organ prolapse and incontinence.
Pelvic Floor Anatomy and Function - The Core Support
- Muscular sling supporting pelvic viscera (bladder, uterus, rectum).
- Pelvic Diaphragm: Forms pelvic floor.
- Levator Ani: Major part.
- Puborectalis: U-shaped; key for anorectal angle & fecal continence.
- Pubococcygeus: Pubis to coccyx.
- Iliococcygeus: Arcus tendineus to coccyx.
- Coccygeus (Ischiococcygeus): Posterior; ischial spine to sacrum/coccyx.
- Levator Ani: Major part.
- Innervation: Pudendal nerve (S2-S4), direct sacral branches.
- Functions: Organ support, continence (urinary/fecal), aids childbirth, defecation, sex.
⭐ Injury to Levator Ani (esp. pubococcygeus, puborectalis) during vaginal delivery is a major risk for pelvic organ prolapse & incontinence.
Pelvic Floor Anatomy and Function - The Front Line
- Urogenital Triangle: Anterior perineum. Houses external genitalia, urethral & vaginal openings.
- Perineal Membrane:
- Dense fascia inferior to urogenital diaphragm. Closes urogenital hiatus anteriorly.
- Supports urethra, vagina; anchors erectile tissues (clitoris/penile bulb).
- Perineal Body (Central Tendon):
- Central fibromuscular mass. Between vagina/penile bulb and anus.
- Crucial for posterior vaginal support, prevents prolapse. 📌 PBS: Perineal Body Support.
⭐ Perineal body: convergence for Bulbospongiosus, EAS, Transverse Perineals, parts of Levator Ani.
Pelvic Floor Anatomy and Function - The Support Network
- Connective Tissue Framework: Synergizes with muscles; vital for organ integrity and position.
- Endopelvic Fascia: Fibroareolar sheath: collagen, elastin, smooth muscle.
- Pubocervical fascia: Supports anterior vaginal wall & bladder.
- Rectovaginal fascia: Supports posterior vaginal wall & rectum.
- Pelvic Ligaments: Key condensations of endopelvic fascia providing suspension.
- Cardinal Ligaments (Transverse Cervical): Primary support for uterus & upper vagina.
- Uterosacral Ligaments: Suspend cervix & upper vagina posteriorly to sacrum.
- Endopelvic Fascia: Fibroareolar sheath: collagen, elastin, smooth muscle.
- DeLancey's Levels of Vaginal Support: Critical 3-tier anatomical model.
Loading diagram…
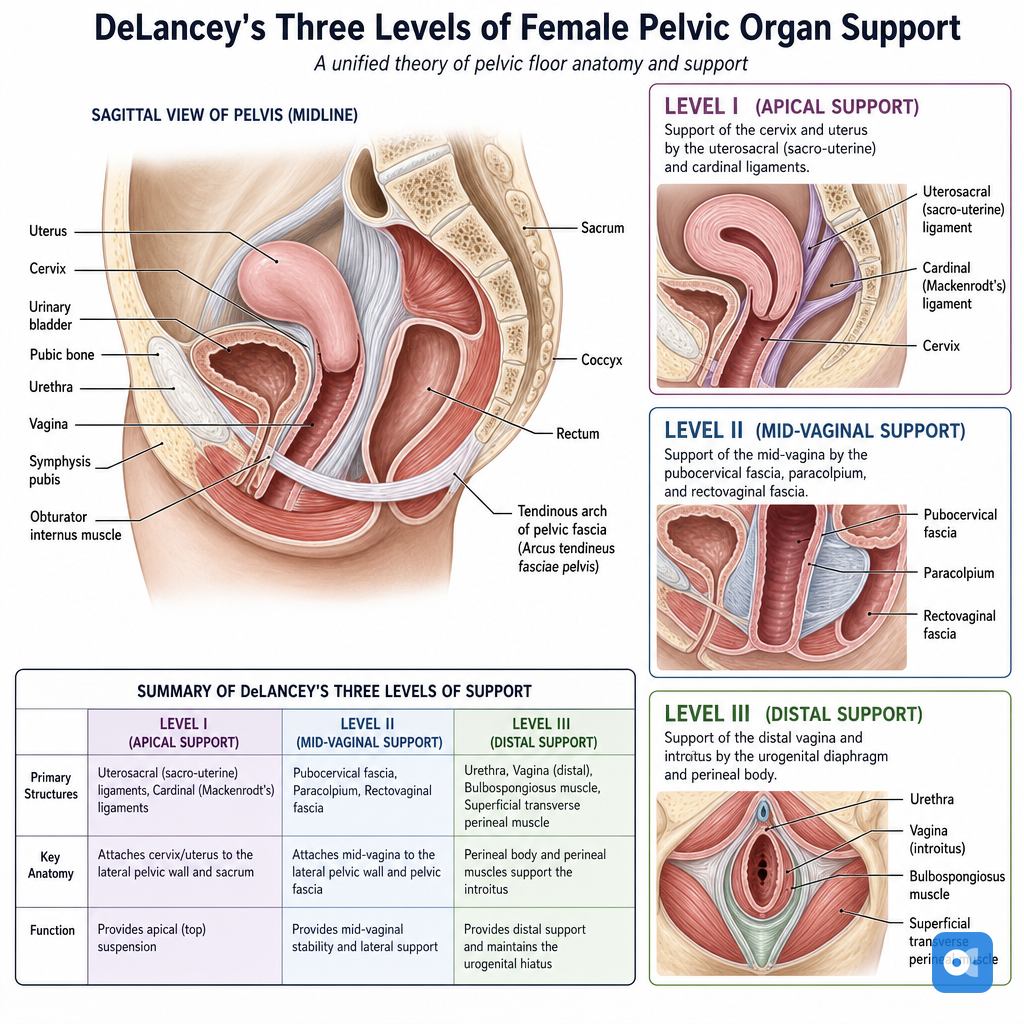
> ⭐ Level I defects (uterosacral-cardinal complex) are the most common cause of uterine or vault prolapse.
Pelvic Floor Anatomy and Function - Nerves & Problems
- Nerve Supply:
- Pudendal Nerve (S2-S4): Primary motor to external sphincters (urethral, anal); sensory to perineum. 📌 S2,3,4 keeps the Pudenda off the floor.
- Levator Ani Nerve (S3-S4): Direct motor to levator ani muscles.
- Autonomic Nerves: Sympathetic (hypogastric plexus) & Parasympathetic (pelvic splanchnic, S2-S4) control bladder/bowel function.
- Common Problems (Dysfunctions):
- Urinary Incontinence (Stress, Urge)
- Fecal Incontinence
- Pelvic Organ Prolapse (POP)
- Sexual Dysfunction
- Chronic Pelvic Pain
⭐ Pudendal nerve injury (e.g., childbirth, cycling) can lead to fecal/urinary incontinence, perineal pain, or sexual dysfunction.
High‑Yield Points - ⚡ Biggest Takeaways
- Levator ani muscles form the pelvic diaphragm, providing primary pelvic support.
- Pudendal nerve (S2-S4): key for perineal sensation & external sphincter motor control.
- Endopelvic fascia: provides crucial connective tissue (suspensory) support for pelvic organs.
- DeLancey's Levels: Level I (apical suspension), Level II (mid-vaginal attachment), Level III (distal fusion) define vaginal support.
- Perineal body: central fibromuscular structure for posterior pelvic floor integrity.
- Intact pelvic floor function: essential for organ support, urinary/fecal continence, and sexual function.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more