

Hypertension - Pressure Cooker Pregnancy
- Gestational HTN: BP ≥140/90 mmHg after 20 wks gestation; no proteinuria.
- Pre-eclampsia: BP ≥140/90 mmHg after 20 wks + Proteinuria (≥300mg/24h or ≥1+ dipstick).
- Severe Pre-eclampsia: BP ≥160/110 mmHg OR end-organ damage (e.g., thrombocytopenia <100,000/µL, ↑LFTs, renal insufficiency, pulm. edema, new visual/CNS sx).
- Eclampsia: Pre-eclampsia + New-onset grand mal seizures.
- HELLP Syndrome: 📌 Hemolysis, Elevated Liver enzymes, Low Platelets. Key Management:
- Antihypertensives (BP goal <160/110 mmHg): Labetalol, Nifedipine, Methyldopa. (Avoid ACEi/ARBs).
- MgSO4 for seizure prophylaxis (severe pre-eclampsia) & treatment (eclampsia):
- Loading dose: 4-6g IV over 15-20 min.
- Maintenance: 1-2g/hr IV.
⭐ MgSO4 is the drug of choice for seizure prophylaxis and control in eclampsia; its therapeutic range is 4-7 mEq/L. Antidote: Calcium gluconate.
- Definitive treatment: Delivery. Complications: Maternal (abruption, DIC, CVA, organ failure), Fetal (IUGR, prematurity, IUD).

GDM - Sugar Spike Saga
- Screening: Universal (DIPSI: 75g OGTT, non-fasting) or risk-based.
- Diagnosis (IADPSG/WHO): ≥1 abnormal value from 75g OGTT:
- Fasting: ≥ 92 mg/dL
- 1-hr: ≥ 180 mg/dL
- 2-hr: ≥ 153 mg/dL
- Complications:
- Maternal: Pre-eclampsia, polyhydramnios, ↑ C-section.
- Fetal: Macrosomia, IUGR, RDS, neonatal hypoglycemia.
- Management:
- MNT (Medical Nutrition Therapy) first.
- OHAs: Metformin (preferred), Glibenclamide (caution).
- Insulin: If targets unmet (Target HbA1c <6.5%).
⭐ India's DIPSI (Diabetes in Pregnancy Study Group India) recommends a one-step procedure with 75g oral glucose load for GDM diagnosis, irrespective of last meal.
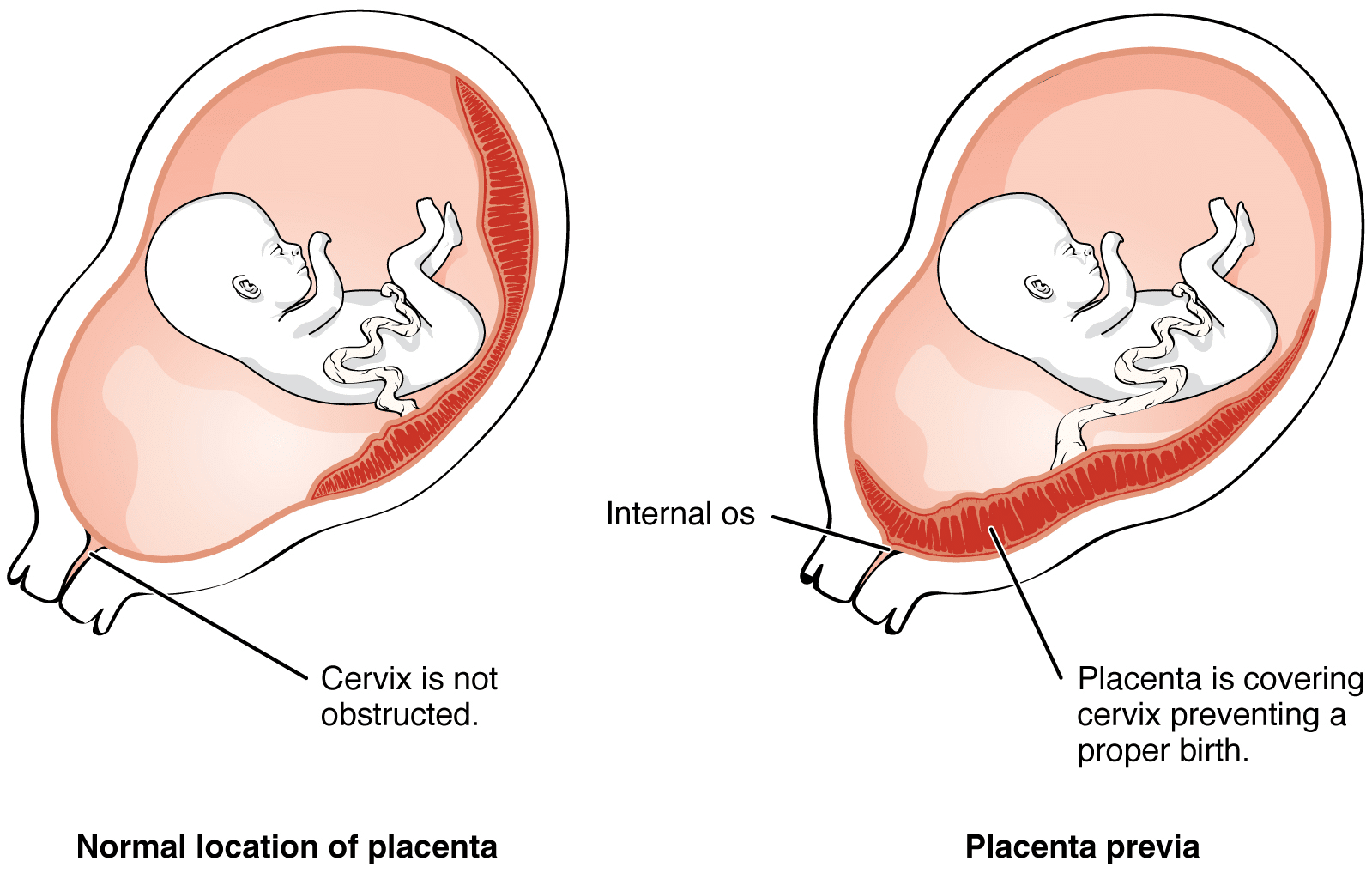
APH - Code Red Bleeds
| Feature | Placenta Previa | Abruptio Placentae |
|---|---|---|
| Bleeding | Painless, causeless, recurrent, bright red | Painful, dark red; may be concealed |
| Uterus | Soft, non-tender | Tender, rigid (hypertonic), "woody" feel |
| Fetal Heart | Usually normal until severe bleed/labor | Fetal distress common & early |
* Types: Complete (covers os), Partial, Marginal (edge at os), Low-lying (near os).
- Abruptio Placentae: Premature separation of a normally implanted placenta.
- Risk Factors:
- Previa: Prior C-section, multiparity, AMA, smoking.
- Abruptio: Maternal HTN, trauma, smoking, cocaine, prior abruption.
- Management Principles:
- Expectant: Stable, preterm (<37 wks). Corticosteroids for fetal lung maturity.
- Active: Term (≥37 wks), maternal/fetal instability, significant bleeding → Prompt delivery (often LSCS for previa; LSCS for fetal distress in abruption).
- Couvelaire Uterus: Extravasation of blood into uterine musculature in severe abruption; uterus appears bruised, woody.
- ⭐ > In Placenta Previa, per-vaginal (PV) examination is contraindicated until placenta location is confirmed by ultrasound to avoid catastrophic hemorrhage.
Preterm & PROM - Tiny Timers
- Definitions:
- Preterm Labor (PTL): Regular contractions + cervical changes <37 weeks.
- PROM: Rupture of membranes before labor onset.
- PPROM: Preterm PROM, <37 weeks.
- Risk Factors: Prior PTL, infection, multiple gestation, cervical insufficiency.
- Diagnosis: Clinical (cervical changes), +fFN, USG Cervical Length (CL) <25mm.
- Management:
- Tocolytics: Delay delivery. Nifedipine, Atosiban. Indomethacin <32 wks (max 48h). 📌 IT'S NOT MY TIME (Indomethacin, Nifedipine, MgSO4, Terbutaline, Atosiban).
- Antenatal Corticosteroids (ACS): Betamethasone 12mg IM x2 (24h apart) or Dexamethasone. Lung maturity (24-34 wks).
- MgSO4: Fetal neuroprotection if imminent delivery <32 weeks.
- Antibiotics: For PPROM (latency) & Group B Strep (GBS) prophylaxis.
⭐ ACS (Betamethasone) significantly ↓ RDS, IVH, NEC in preterms (24-34 wks).
Loading diagram…
High‑Yield Points - ⚡ Biggest Takeaways
- Gestational Diabetes Mellitus (GDM): Screen with OGTT; manage with diet, exercise, insulin.
- Preeclampsia: Hypertension (>140/90 mmHg) & proteinuria after 20 weeks; MgSO4 for seizure prophylaxis.
- Ectopic Pregnancy: Suspect with amenorrhea, pain, bleeding; β-hCG & transvaginal ultrasound (TVS) are key.
- Placenta Previa: Painless third-trimester bleeding; avoid per-vaginal (PV) exams.
- Abruptio Placentae: Painful vaginal bleeding, uterine tenderness; risk of fetal distress.
- Intrauterine Growth Restriction (IUGR): Monitor with serial ultrasounds (USG) & Doppler studies.
- Rh Isoimmunization: Administer Anti-D immunoglobulin at 28 weeks & post-delivery for Rh-negative mothers with Rh-positive babies.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more