

Shock: Definition & Types - The Basics Blitz
Shock: Cellular hypoxia from inadequate tissue perfusion.
-
Stages of Shock:
- Compensated: Tachycardia, vasoconstriction maintain BP; cool peripheries.
- Progressive: Hypotension, oliguria, acidosis, altered mental status.
- Irreversible: Anuria, profound hypotension, coma, MODS; often fatal.
-
Classification & Hemodynamic Profiles:
Type Common Causes CO SVR PCWP CVP Hypovolemic Hemorrhage, burns, dehydration ↓ ↑ ↓ ↓ Cardiogenic MI, acute MR/VSD, arrhythmia, cardiomyopathy ↓ ↑ ↑ ↑ Distributive Systemic Vasodilation - Septic Infection + SIRS ↑/↔ ↓ ↔/↓ ↔/↓ - Anaphylactic IgE-mediated; drugs, venom ↓ ↓ ↓ ↓ - Neurogenic Spinal injury (≥T6), high spinal ↓ ↓ ↓ ↓ Obstructive Tamponade, massive PE, tension pneumo ↓ ↑ ↔/↑ ↑
⭐ In neurogenic shock, bradycardia may occur despite hypotension due to loss of sympathetic tone. 📌 (Unopposed Vagal Tone)
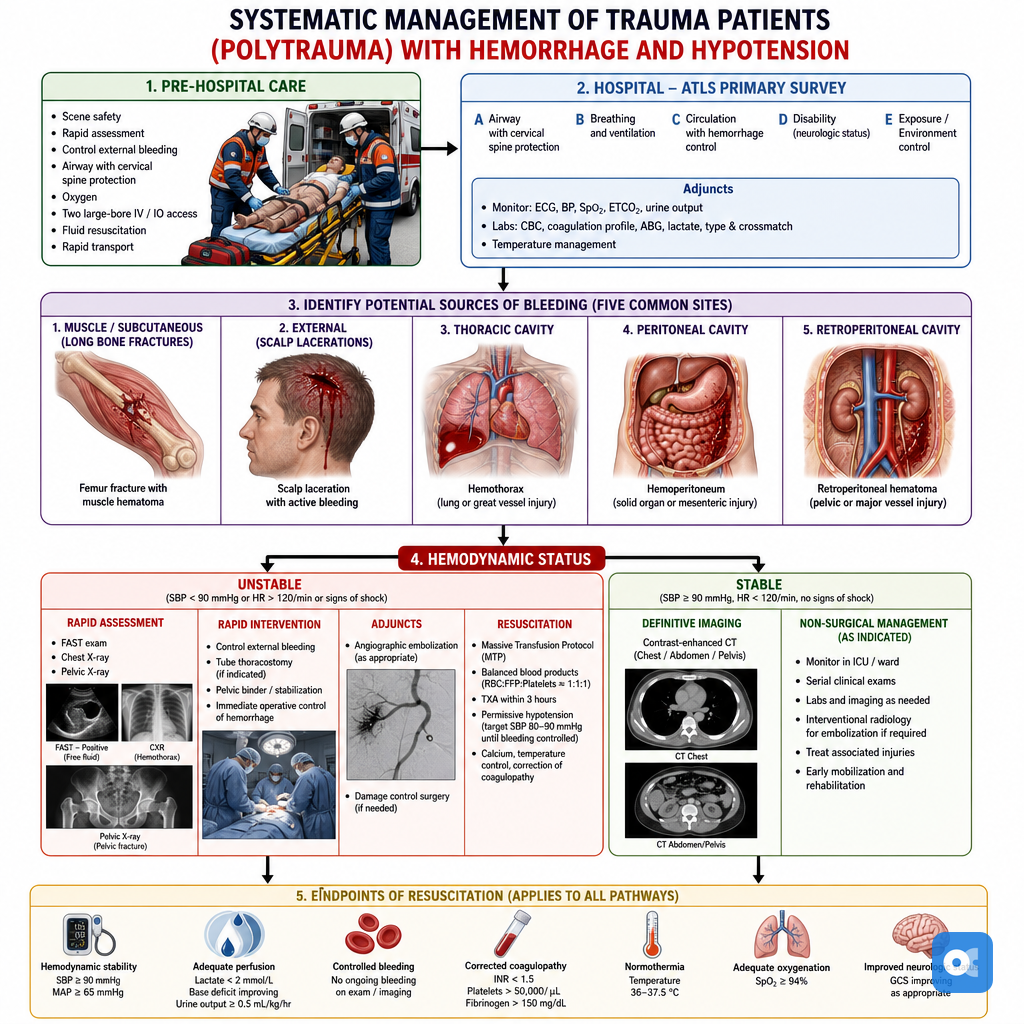
Hemorrhagic Shock: Trauma Focus - Trauma's Red Alert
- Initial Assessment & Recognition:
- ABCDE approach (Airway, Breathing, Circulation, Disability, Exposure).
- Recognize shock: Tachycardia (often earliest sign), hypotension (late sign), tachypnea, altered mental status, cool/clammy skin, ↓ urine output (<0.5 mL/kg/hr).
- FAST scan (Focused Assessment with Sonography for Trauma) for internal bleeding.
- Lethal Triad: Acidosis, Coagulopathy, Hypothermia (📌 A-C-H: "Aches" in trauma).
ATLS Classification of Hemorrhagic Shock:
| Class | Blood Loss (%) | HR (bpm) | BP | RR (bpm) | Mental Status | Fluid Replacement |
|---|---|---|---|---|---|---|
| I | <15% | <100 | Normal | 14-20 | Sl. Anxious | Crystalloid |
| II | 15-30% | >100 | Normal/↓ | 20-30 | Mildly Anxious | Crystalloid |
| III | 30-40% | >120 | ↓ | 30-40 | Anxious/Confused | Crystalloid+Blood |
| IV | >40% | >140 | Marked ↓ | >35 | Confused/Leth. | Blood+Crystalloid |
| %%{init: {'flowchart': {'htmlLabels': true}}}%% | ||||||
| flowchart TD |
Start["⚠️ Trauma Patient
• Suspect hemorrhage• Assess stability"]
Survey["📋 Primary Survey
• ABCDE protocol• Rapid assessment"]
Bleed["🩸 Bleeding Control
• Apply pressure• Tourniquet if needed"]
Access["💊 IV Access
• 2x large bore IVs• IO if IV fails"]
Fluids["💊 Initial Fluids
• Warm crystalloids• 1L bolus dose"]
Assess["📋 Assess Response
• Vitals and FAST• Lactate deficit"]
MTP["⚠️ Activate MTP
• Massive transfusion• Blood products"]
Care["✅ Definitive Care
• Continued support• Surgical repair"]
Start --> Survey Survey --> Bleed Bleed --> Access Access --> Fluids Fluids --> Assess
Assess -->|Response| Care Assess -->|No Response| MTP MTP --> Care
style Start fill:#FDF4F3, stroke:#FCE6E4, stroke-width:1.5px, rx:12, ry:12, color:#B91C1C style Survey fill:#FEF8EC, stroke:#FBECCA, stroke-width:1.5px, rx:12, ry:12, color:#854D0E style Bleed fill:#FDF4F3, stroke:#FCE6E4, stroke-width:1.5px, rx:12, ry:12, color:#B91C1C style Access fill:#F1FCF5, stroke:#BEF4D8, stroke-width:1.5px, rx:12, ry:12, color:#166534 style Fluids fill:#F1FCF5, stroke:#BEF4D8, stroke-width:1.5px, rx:12, ry:12, color:#166534 style Assess fill:#FEF8EC, stroke:#FBECCA, stroke-width:1.5px, rx:12, ry:12, color:#854D0E style MTP fill:#FDF4F3, stroke:#FCE6E4, stroke-width:1.5px, rx:12, ry:12, color:#B91C1C style Care fill:#F6F5F5, stroke:#E7E6E6, stroke-width:1.5px, rx:12, ry:12, color:#525252
> ⭐ In trauma, a base deficit > **-6** mEq/L on ABG is a strong indicator of significant hemorrhage and shock, correlating with increased mortality.
## Resuscitation Rally - The Fluid Fight
**Damage Control Resuscitation (DCR) Principles:**
* Permissive Hypotension: SBP **80-90 mmHg** (SBP >**110 mmHg** if TBI for CPP). Avoid over-resuscitation.
* Hemostatic Resuscitation: Early blood products (PRBC:FFP:PLT ~**1:1:1**) for coagulopathy.
* Lethal Triad Prevention (📌 Hypothermia <**35°C**, Acidosis pH <**7.2**, Coagulopathy):
- Actively warm patient & fluids.
- Optimize perfusion; use balanced crystalloids.
- Early products, TXA, Ca++; guide with TEG/ROTEM.
**Fluid Choices:**
* Crystalloids: Balanced (LR/Plasmalyte) > NS. Limit volume.
* Colloids: Limited role.
**Massive Transfusion Protocol (MTP):**
* Triggers: ABC score ≥**2**, Class III/IV shock, specific injuries, gestalt.
* Ratio: PRBC:FFP:Platelets **1:1:1** (ideal) or **1:1:2**. Mimics whole blood.
* TXA: **1g** IV load <3hrs injury, then **1g**/8hrs infusion.
* Calcium: Monitor & replete IV (citrate binds Ca++).
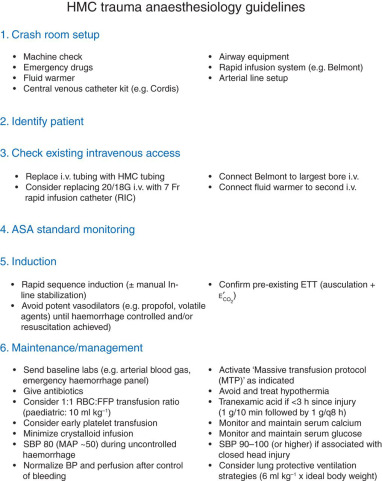
**Vasopressors/Inotropes:**
* Norepinephrine: For refractory hypotension (MAP <**65 mmHg**) post-volume.
* Inotropes: If cardiac dysfunction.
**Endpoints of Resuscitation:**
* Urine Output: >**0.5 ml/kg/hr**.
* Lactate/Base Deficit: Normalize.
* ScvO2: >**70%**.
* Hemodynamics: Stable.
> ⭐ Early TXA (**1g** IV <3 hrs injury, then **1g**/8 hrs) reduces bleeding mortality in trauma.
## High‑Yield Points - ⚡ Biggest Takeaways
> * **Hemorrhagic shock** is the most common cause in trauma; **Class III/IV** requires aggressive resuscitation.
> * **Permissive hypotension** (target SBP **80-90 mmHg**) is crucial in penetrating trauma without **traumatic brain injury (TBI)** until bleeding is controlled.
> * **Massive Transfusion Protocol (MTP)** aims for a balanced resuscitation with a **1:1:1 ratio** of PRBCs:FFP:Platelets.
> * Administer **Tranexamic Acid (TXA)** within **3 hours** of injury in bleeding trauma patients to reduce mortality.
> * Actively prevent and treat the **"lethal triad"** of trauma: **hypothermia, acidosis, and coagulopathy**.
> * **Goal-directed resuscitation** utilizes endpoints like lactate clearance, base deficit, and urine output to guide therapy effectively.
> * Early **calcium replacement** is vital during massive transfusions to prevent citrate-induced hypocalcemia and myocardial depression.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more