

AUB: Basics & PALM-COEIN - Decoding the Drip
- AUB: Abnormal Uterine Bleeding - deviation from normal menstrual cycle (frequency, regularity, duration, volume).
- Normal: Cycle 21-35 days, duration ≤7 days, volume 5-80 mL.
- Key Patterns:
- Heavy Menstrual Bleeding (HMB): >80 mL/cycle or >7 days, or impacting QoL.
- Intermenstrual Bleeding (IMB): Bleeding between menses.
- PALM-COEIN (FIGO Classification): 📌
- PALM (Structural):
- Polyp (AUB-P)
- Adenomyosis (AUB-A)
- Leiomyoma (AUB-L)
- Malignancy/Hyperplasia (AUB-M)
- COEIN (Non-Structural):
- Coagulopathy (AUB-C)
- Ovulatory Dysfunction (AUB-O)
- Endometrial (AUB-E)
- Iatrogenic (AUB-I)
- Not Yet Classified (AUB-N)
- PALM (Structural):

⭐ AUB-O (Ovulatory dysfunction) is the most common cause of AUB, particularly at extremes of reproductive age.
AUB: Etiology In-Depth - Cause Code Crackdown
PALM (Structural)
- Polyp: Endometrial/cervical. Intermenstrual/postcoital bleeding.
- Adenomyosis: Endometrial tissue in myometrium. HMB, dysmenorrhea, tender bulky uterus.
- Leiomyoma: Fibroids. Submucosal type most often causes AUB.
- Malignancy/Hyperplasia: Endometrial cancer (esp. PMB). Biopsy >45 yrs or risk factors.
COEIN (Non-Structural)
- Coagulopathy: Von Willebrand disease (commonest). Screen if HMB from menarche/family Hx.
- Ovulatory Dysfunction: PCOS, thyroid, stress → unopposed estrogen → irregular, heavy bleeding.
- Endometrial: Local factors (e.g., endometritis). Diagnosis of exclusion.
- Iatrogenic: Hormonal contraception (breakthrough), anticoagulants, copper IUDs.
- Not Classified: Rare (AVMs, C-section scar defect/isthmocele).
⭐ Up to 20% of adolescents with severe AUB have a coagulopathy, often Von Willebrand disease.
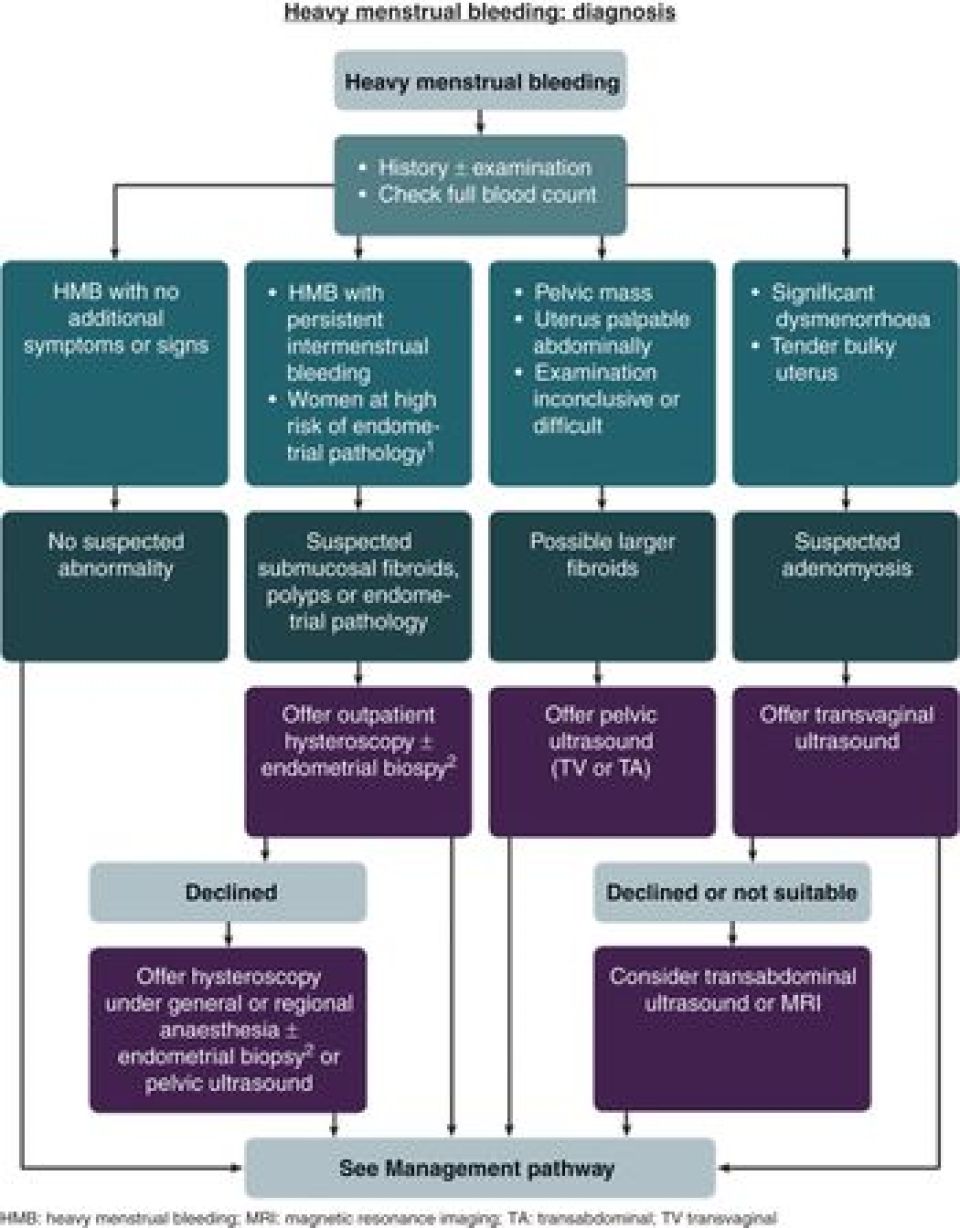
AUB: Diagnostic Approach - Sleuthing the Source
- History: Menstrual (LMP, cycle, flow, IPB, PCB), medical, family Hx (bleeding disorders, cancer).
- Examination: General (pallor, BMI, thyroid), P/A, P/S & P/V (source, uterine size, adnexa).
- Investigations (guided by PALM-COEIN framework):
- Labs: CBC, β-hCG, TSH. Coagulation profile if indicated.
- Imaging: TVS (1st line). SIS for better endometrial view.
- Endometrial Sampling: Biopsy if >45 yrs, risk factors (obesity, PCOS), persistent AUB, failed Rx.
- Hysteroscopy: Gold standard for intrauterine pathology.
Loading diagram…
> ⭐ Endometrial sampling is crucial for women >**45** years with AUB to exclude endometrial hyperplasia or carcinoma.
AUB: Management Strategies - Taming the Tide
- Acute AUB:
- Assess hemodynamic stability: IV fluids, urgent blood transfusion if Hb < 7 g/dL.
- Medical (rapid control):
- High-dose IV Estrogen (CEE 25 mg q4-6h).
- High-dose Progestins (MPA 20 mg TID).
- Tranexamic acid (1.3 g PO / 10 mg/kg IV TID, max 600mg/dose).
- High-dose OCPs (tapering regimen).
- Surgical (if medical fails/CI): D&C, hysteroscopy.
- Chronic AUB (PALM-COEIN guided):
- Medical (long-term management):
- Non-hormonal: NSAIDs (during menses), Tranexamic acid.
- Hormonal: OCPs, Progestins (oral, depot, LNG-IUS), GnRH analogs (short-term).
- Surgical (cause-specific/refractory): Endometrial ablation, Myomectomy, Polypectomy, Hysterectomy.
- Medical (long-term management):
⭐ LNG-IUS is first-line for AUB-O and AUB-E in many cases, reducing blood loss by up to 90%.
Loading diagram…
High‑Yield Points - ⚡ Biggest Takeaways
- PALM-COEIN is the primary AUB classification system, guiding diagnosis and management.
- Endometrial sampling is vital for women >45 years or with risk factors for malignancy.
- Ovulatory dysfunction (AUB-O), often linked to PCOS, is a frequent cause.
- Structural lesions (polyps, adenomyosis, leiomyomas) are best identified via ultrasound or hysteroscopy.
- Medical therapy (hormonal, tranexamic acid) is the initial approach for most AUB.
- Heavy Menstrual Bleeding (HMB) is defined as blood loss >80 mL per cycle or lasting >7 days.
- Suspect coagulopathy in adolescents with severe HMB, especially if present since menarche.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more