

Bordetella: Basics & Pathogenesis - Whoop Toxin Terror
- Gram-negative coccobacilli, strictly aerobic.
- B. pertussis causes whooping cough (pertussis).
- Pathogenesis Stages:
- Attachment: Mediated by adhesins (Filamentous hemagglutinin (FHA), pertactin, fimbriae) to ciliated respiratory epithelium.
- Evasion & Damage:
- Pertussis Toxin (PTx): ADP-ribosylates Gi protein → ↑cAMP → lymphocytosis, hypoglycemia, histamine sensitization. (📌 Pertussis Toxin = Permanently Turned on AC)
- Adenylate Cyclase/Hemolysin Toxin: ↑cAMP locally.
- Tracheal Cytotoxin: Damages ciliated cells, impairs clearance.
- Dermonecrotic Toxin: Vasoconstriction.

⭐ Pertussis Toxin (PTx) is the major virulence factor, responsible for the characteristic paroxysmal cough and systemic manifestations like profound lymphocytosis (WBC often > 20,000/μL, mostly lymphocytes).
Bordetella: Clinical & Management - Cough Cure Quest
- Clinical Presentation (Whooping Cough):
- Catarrhal Stage (1-2 wks): Rhinorrhea, malaise, mild cough; highly contagious.
- Paroxysmal Stage (2-8 wks): Intense coughing fits, inspiratory "whoop", post-tussive vomiting, lymphocytosis.
- Convalescent Stage (wks-months): Gradual recovery, lingering cough.
- Diagnosis:
- Nasopharyngeal swab/aspirate: PCR (gold standard, esp. first 3 wks), Culture (Regan-Lowe/Bordet-Gengou agar; charcoal blood agar).
- Serology: Useful later in illness.
- Management:
- Macrolides: Azithromycin, Erythromycin, Clarithromycin (effective in catarrhal stage to ↓ severity & spread).
- Supportive care: Oxygen, hydration.
- Prophylaxis for close contacts.
- Complications: Pneumonia, otitis media, seizures, encephalopathy.
⭐ Marked lymphocytosis is a characteristic finding in the paroxysmal stage of pertussis.
Loading diagram…
Brucella: Basics & Pathogenesis - Fever Agent Antics
- Gram-negative coccobacilli; aerobic, non-motile, non-sporing.
- Biochemical markers: Catalase (+), Oxidase (+), rapid Urease (+). (📌 Urease helps differentiate)
- Zoonotic disease: Causes Undulant fever (Malta fever, Bang's disease).
- Transmission: Unpasteurized dairy, animal contact, aerosols.
- Pathogenesis: Facultative intracellular parasite (macrophages of RES).
- Evades killing: Inhibits phagolysosome fusion for intracellular survival.
- Virulence: Type IV secretion system (VirB) is essential.
- Pathology: Forms non-caseating granulomas.
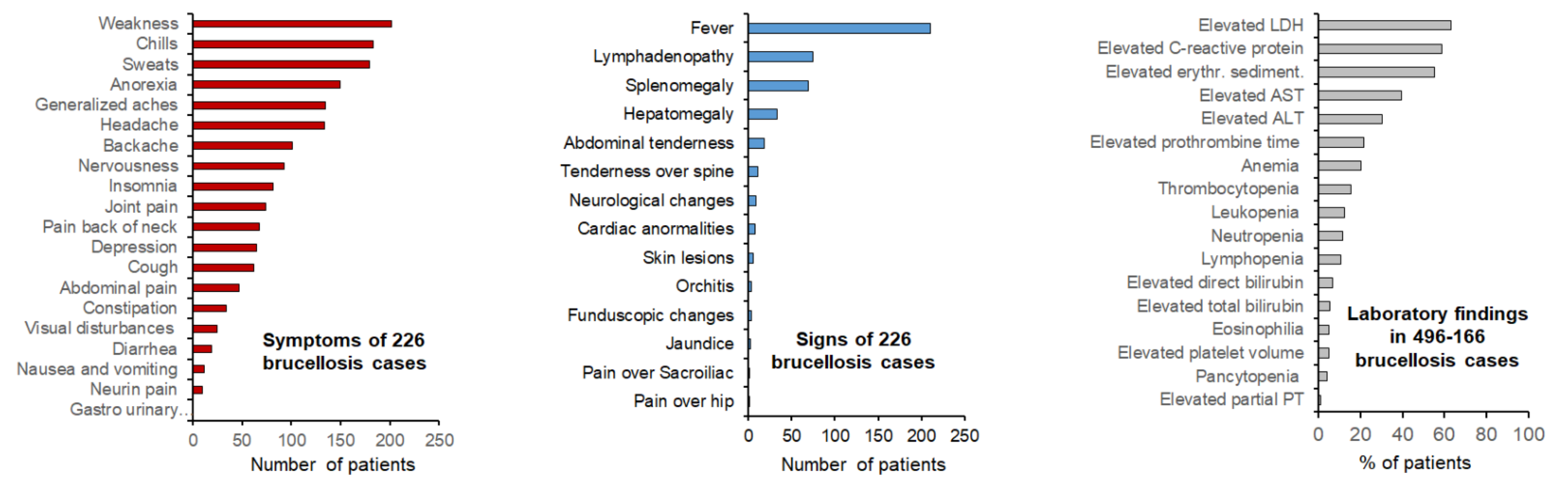
- Clinical: Undulant fever, drenching sweats, arthralgia, hepatosplenomegaly.
⭐ Brucella's hallmark is undulant fever, a relapsing febrile illness reflecting its persistence within the reticuloendothelial system, often acquired from unpasteurized milk.
Brucella: Clinical & Management - Brucella Battle Plan
- Clinical: Insidious onset.
- Systemic: Undulant fever (cyclical), drenching sweats (mouldy odor), malaise, arthralgia.
- Focal (common): Hepatosplenomegaly. Osteoarticular (sacroiliitis, spondylitis - most frequent, ~30-70%). Genitourinary (epididymo-orchitis). Neurobrucellosis (<5%). Endocarditis (rare, high mortality).
- Diagnosis:
- Culture: Blood/BM (Gold Std; Castaneda’s medium, prolonged incubation 4-6w).
- Serology: SAT ≥1:160 (non-endemic) or ≥1:320 (endemic)/4-fold rise. 2-ME (IgG, active). Coombs (non-agglutinating Abs). ELISA.
- PCR: Rapid.
- Management: Combination therapy vital.
Loading diagram…
> ⭐ Relapse occurs in **5-15%** of cases, often due to poor adherence or sequestered infection.
High‑Yield Points - ⚡ Biggest Takeaways
- Bordetella pertussis causes whooping cough; its Pertussis toxin ADP-ribosylates Gi, increasing cAMP.
- Culture B. pertussis on Bordet-Gengou or Regan-Lowe media.
- Brucella species cause brucellosis (undulant fever), transmitted by unpasteurized dairy or animal contact.
- Brucella is a facultative intracellular pathogen, leading to granulomas.
- Diagnose brucellosis via blood/bone marrow culture and serology (Rose Bengal, SAT).
- Treat brucellosis with Doxycycline + Rifampicin.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more