

Pediatric Voice - Little Larynxes, Big Sounds
- Pediatric vs. Adult Larynx:
- Size: Smaller in all dimensions.
- Position: Higher (📌 C3-C4 child vs. C5-C6 adult).
- Cartilage: Softer, less calcified, more prone to collapse.
- Subglottic Shape: Funnel-shaped (narrowest at cricoid ring), unlike adult cylindrical shape. This makes children prone to croup.
- Common Symptoms:
- Hoarseness: Most frequent.
- Stridor: High-pitched; inspiratory, expiratory, or biphasic.
- Weak cry or altered cry.
- Aphonia (loss of voice).
- Vocal fatigue with use.
, cartilage consistency, and subglottic shape (funnel vs cylinder))

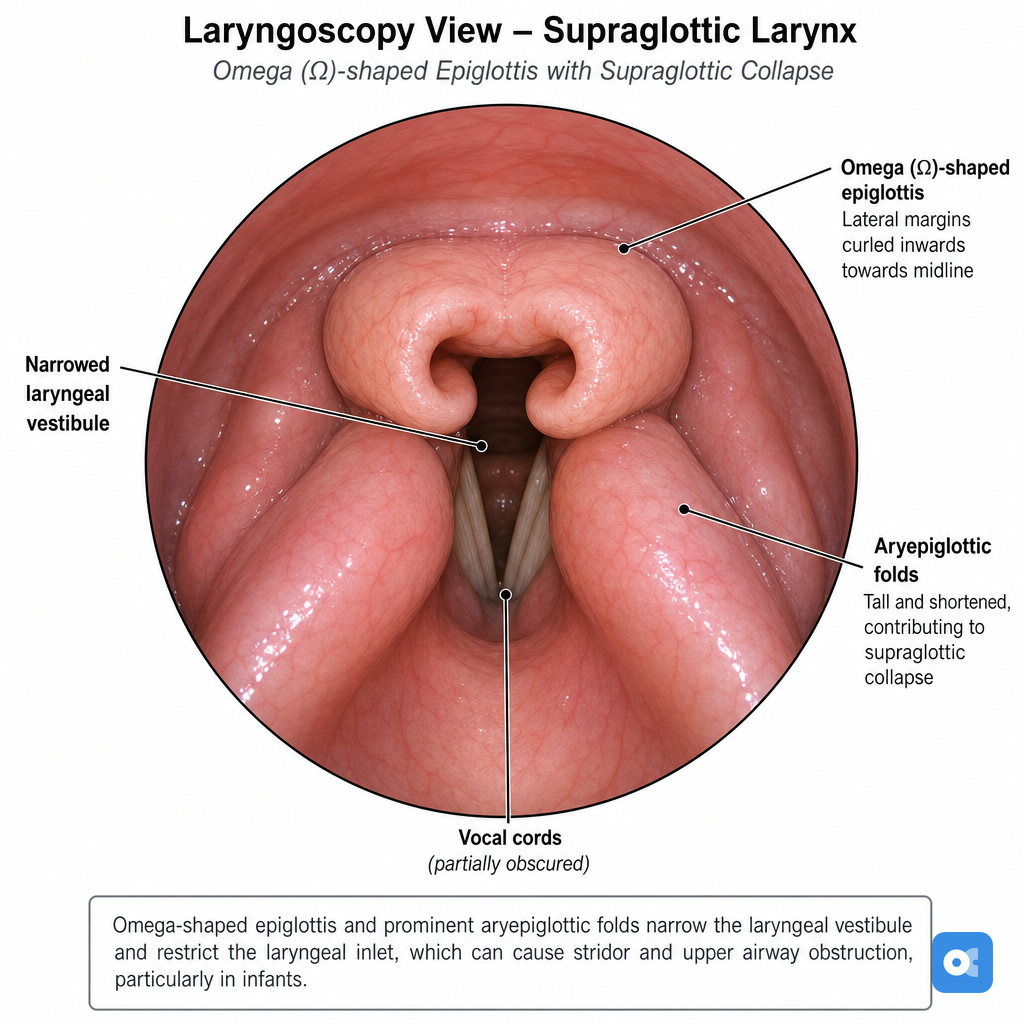
⭐ Laryngomalacia is the most common congenital laryngeal anomaly and cause of stridor in infants.
Congenital Quirks - Built-In Voice Woes
- Laryngomalacia: Commonest cause of infant stridor. Inspiratory stridor, omega-shaped epiglottis.
- Type I: Arytenoid prolapse.
⭐ Type I Laryngomalacia (prolapse of arytenoids) is the most common type.
- Type II: Short aryepiglottic folds.
- Type III: Epiglottic collapse.
- Type I: Arytenoid prolapse.
Loading diagram…
- Congenital Vocal Fold Paralysis:
- Unilateral: Weak cry, aspiration. More common.
- Bilateral: Stridor, airway distress. Causes: birth trauma, CNS.
- Laryngeal Webs: Anterior. Hoarseness/aphonia. Severity: Cohen's classification (Type I-IV).
- Subglottic Stenosis: Congenital (cartilaginous/membranous) or acquired. Biphasic stridor. Cotton-Myer Grade I-IV.
- Laryngeal Cysts:
- Saccular: From saccule; airway obstruction risk.
- Ductal: Mucous retention on TVF.
- Sulcus Vocalis: Groove on VF edge; hoarse, breathy voice.
Acquired Issues - Voice Under Pressure
| Feature | Vocal Nodules | Vocal Polyps |
|---|---|---|
| Laterality | Bilateral (📌 'Naughty') | Unilateral (📌 'Peculiar') |
| Etiology | Chronic voice abuse | Acute/chronic voice abuse |
| Appearance | Small, symmetric, whitish | Larger, hemorrhagic/gelatinous |
| Location | Anterior 1/3 - Mid 2/3 vocal fold junction | Mid-cord, often unilateral |
- Cause: HPV **6** & **11**.
- Lesions: Multiple, wart-like lesions on larynx/airway.
- Tx: Surgery ± Cidofovir.
- Functional Dysphonia
- Cause: Psychogenic or Muscle Tension Dysphonia (MTD).
- Voice: Strained, breathy, or aphonia; no organic lesion.
- Puberphonia (Mutational Falsetto)
- Issue: Persistently high-pitched male voice after puberty (falsetto).
- Tx: Voice therapy.
⭐ Vocal nodules are the most common cause of persistent hoarseness in school-aged children.
Dx & Rx - Tuning Tiny Tones
-
Diagnosis (Dx):
- History: Crucial details: onset, nature of cry/voice, feeding difficulties, respiratory distress.
- Examination:
- Perceptual Voice Evaluation: GRBAS/CAPE-V scales.
- Laryngeal Visualization:
- Flexible Nasopharyngolaryngoscopy (FNPL): Primary diagnostic tool.
⭐ Flexible nasopharyngolaryngoscopy is the primary diagnostic tool for visualizing laryngeal pathology in children.
- Rigid Laryngoscopy: Detailed views, often under GA.
- Stroboscopy: Assesses vocal fold vibration if cooperation allows.
- Flexible Nasopharyngolaryngoscopy (FNPL): Primary diagnostic tool.
- Objective Assessment: Acoustic analysis (F0, jitter, shimmer), aerodynamic measures (MPT).
-
Treatment (Rx) Strategy:
Loading diagram…
* **Management Pillars:**
- **Voice Therapy:** Cornerstone for vocal nodules, functional disorders; age-specific techniques.
- **Medical:** GERD treatment; Antivirals for RRP (e.g., Cidofovir).
- **Surgical (MLS):** For congenital webs, cysts, severe RRP, or failed conservative treatment.
High‑Yield Points - ⚡ Biggest Takeaways
- Laryngomalacia: Most common cause of infantile stridor; typically inspiratory.
- Vocal Nodules: Most frequent cause of chronic hoarseness in children; due to voice abuse.
- RRP (Recurrent Respiratory Papillomatosis): Caused by HPV 6 & 11; hoarseness, stridor.
- Subglottic Stenosis: Congenital or acquired; presents with biphasic stridor.
- Vocal Cord Paralysis: Unilateral leads to weak cry/hoarseness; bilateral causes stridor/respiratory distress.
- Laryngeal Webs: Congenital; cause hoarseness/aphonia from birth.
- Voice Therapy: Key for functional voice disorders like nodules.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more