

Definition & Classification - Sinus Siege Saga
- CRS: Nasal & paranasal sinus inflammation ≥12 weeks.
- Symptoms (≥2, one primary):
- Primary: Nasal blockage/congestion OR nasal discharge (anterior/posterior).
- Secondary: Facial pain/pressure OR hyposmia/anosmia.
- Objective evidence: Endoscopic signs (polyps, mucopurulent discharge, edema) OR CT changes.
- EPOS Types:
- CRSwNP (with Nasal Polyps)
- CRSsNP (without Nasal Polyps)
⭐ The 12-week duration is crucial for differentiating chronic from acute or subacute rhinosinusitis.
Pathophysiology & Etiology - The Blockade Builders
- Multifactorial: persistent inflammation, microbial infection, impaired mucociliary clearance.
- Key trigger: Obstruction of sinus ostia, especially the Ostiomeatal Complex (OMC).
- Etiological factors:
- Anatomical: Septal deviation, concha bullosa, Haller cells, paradoxical middle turbinate.
- Inflammatory/Immune: Allergic rhinitis, asthma, Aspirin Exacerbated Respiratory Disease (AERD), cystic fibrosis, primary ciliary dyskinesia, immunodeficiency.
- Infectious: Bacterial biofilms (e.g., S. aureus, P. aeruginosa), fungal elements (e.g., Allergic Fungal Rhinosinusitis - AFRS).
- Environmental: Pollutants, tobacco smoke.
- Vicious cycle: Obstruction → Stasis → Hypoxia → Mucosal damage → Inflammation/Infection → Further obstruction.

⭐ The Ostiomeatal Complex (OMC) is the key drainage pathway for frontal, maxillary, and anterior ethmoid sinuses; its obstruction is central to CRS development and persistence.
Clinical Features - The Pressure Plot
- EPOS 2020 Criteria: ≥2 symptoms for ≥12 weeks.
- At least 1 symptom must be:
- Nasal blockage/obstruction/congestion OR
- Nasal discharge (anterior/posterior).
- At least 1 symptom must be:
- Symptoms:
Major (📌 NO FaceS) Minor Nasal Obstruction/Blockage Headache Olfactory Dysfunction (Hyposmia/Anosmia) Halitosis Facial Pain/Pressure Fatigue Anterior/Posterior Nasal Discharge Dental Pain Cough Ear Pain/Pressure/Fullness
⭐ Nasal obstruction/blockage/congestion and nasal discharge (anterior/posterior) are key major symptoms for diagnosis according to EPOS guidelines.
(NO FaceS: Nasal Obstruction, Olfactory dysfunction, Facial pain/pressure, Secretions/Discharge)
Diagnosis & Investigations - Detective Work
- Nasal Endoscopy: Visualizes polyps, discharge, edema. Key initial step.
- Imaging & Staging:
Loading diagram…
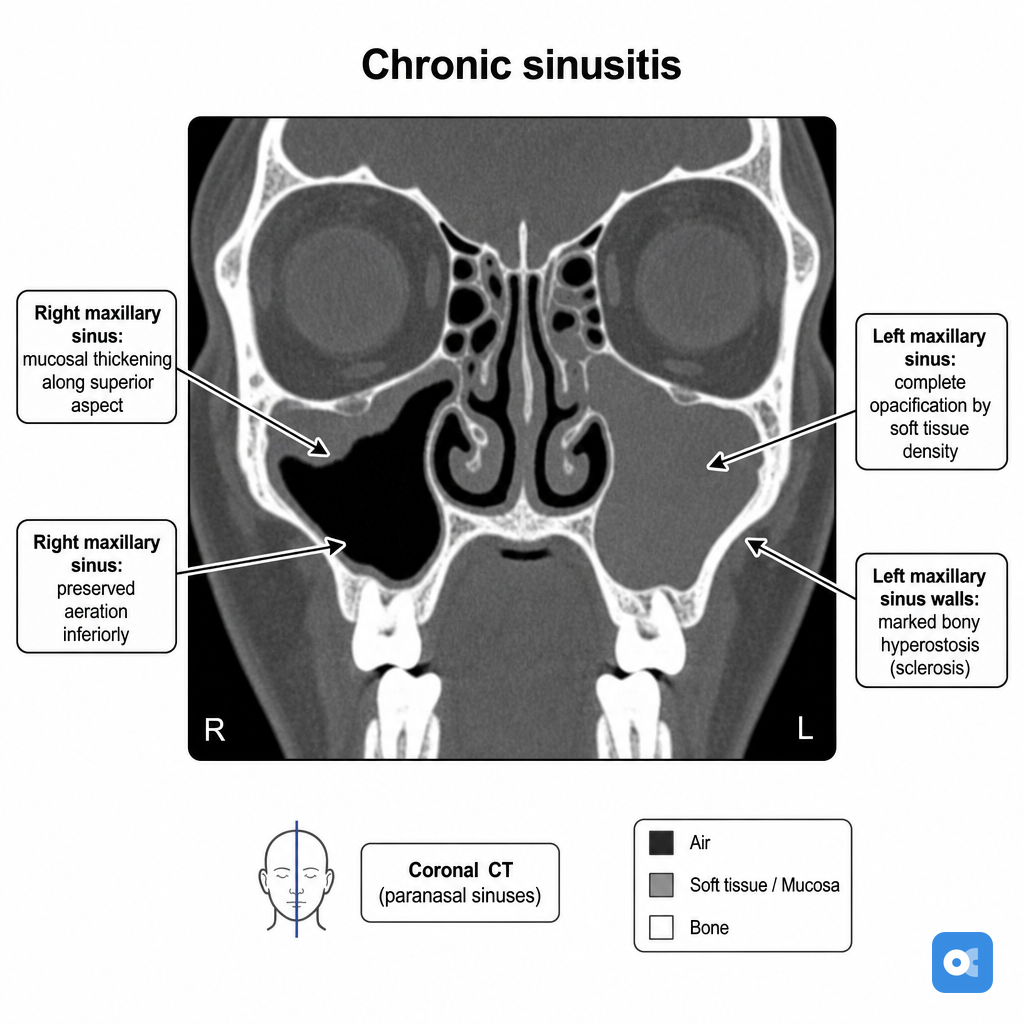
> ⭐ **Non-contrast CT scan of paranasal sinuses (NCCT PNS)** is the gold standard imaging for CRS evaluation.
- Ancillary Tests:
- Allergy testing (skin prick, IgE) if suspicion of allergic component.
- Biopsy for unilateral disease, suspected fungal, or neoplasm.
Management - Clearing the Path
- Goal: ↓inflammation, ↑drainage, eradicate infection, ↓symptoms.
- Medical First:
- Intranasal corticosteroids (INS): Long-term; e.g., fluticasone, mometasone.
- Saline irrigation: Daily, high-volume.
- Oral corticosteroids (OCS): Short bursts (e.g., prednisolone 0.5mg/kg, 5-10 days) for severe exacerbations/polyps.
- Antibiotics: For acute bacterial exacerbations; not routine.
- Biologics (e.g., Dupilumab): Severe CRSwNP refractory to OCS/surgery.
- Surgical:
- Functional Endoscopic Sinus Surgery (FESS): If medical therapy fails or complications.
⭐ Intranasal corticosteroids are the cornerstone of medical management for all types of CRS.
Loading diagram…
Complications - Danger Zones
- Orbital (Most Common): Chandler's Stages (📌 Mnemonic: "Please Order Some Appetizers Carefully"):
- I: Preseptal cellulitis
- II: Orbital cellulitis
- III: Subperiosteal abscess
- IV: Orbital abscess
- V: Cavernous Sinus Thrombosis (CST)
⭐ Orbital cellulitis (Stage II) = most common orbital complication.
- Intracranial: Meningitis, epidural/subdural/brain abscess, CST.
- Bony: Osteomyelitis (Pott's puffy tumor - frontal).
- Mucocele/Pyocele. oka
High‑Yield Points - ⚡ Biggest Takeaways
- Chronic Rhinosinusitis (CRS): Nasal/sinus inflammation >12 weeks.
- Diagnosis: ≥2 major symptoms (blockage, discharge, facial pain/pressure, hyposmia/anosmia).
- CRSwNP (with polyps): Often eosinophilic, linked to AERD and AFRS.
- AFRS: Allergic mucin with fungal hyphae (no invasion), Charcot-Leyden crystals.
- CT scan is crucial for diagnosis/extent; Lund-Mackay score quantifies.
- Treatment: Intranasal corticosteroids (mainstay); FESS for refractory cases.
- Osteomeatal Complex (OMC) obstruction is a common pathogenic factor.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more