

MV Fundamentals - Breath of Life
Goals of Mechanical Ventilation:
- ↓ Work of Breathing (WOB), reduce muscle fatigue.
- Support adequate gas exchange ($O_2$ uptake, $CO_2$ removal).
- Reverse life-threatening hypoxemia (e.g., $P_aO_2$ < 60 mmHg).
- Reverse acute respiratory acidosis (e.g., pH < 7.25 due to ↑$P_aCO_2$).
Key Indications:
- Apnea or insufficient spontaneous ventilation.
- Acute Respiratory Failure:
- Type I (Hypoxemic): $P_aO_2$ < 60 mmHg despite high $F_iO_2$.
- Type II (Hypercapnic): $P_aCO_2$ > 50 mmHg & pH < 7.25.
- Airway protection (e.g., GCS < 8, risk of aspiration).
- Impending respiratory collapse (e.g., severe distress, muscle fatigue).
- Elective support (e.g., post-operative recovery, certain procedures).
⭐ PEEP (Positive End-Expiratory Pressure) is vital to prevent alveolar collapse (atelectrauma) and improve oxygenation by recruiting alveoli.
Ventilator Modes - Control Freaks & Helpers
- Volume Control (VC): Delivers preset tidal volume ($V_T$); airway pressure ($P_{aw}$) varies. Guarantees minute ventilation. Risk: Barotrauma.
- Pressure Control (PC): Delivers preset inspiratory pressure ($P_{insp}$); $V_T$ varies with lung mechanics. Limits $P_{aw}$. Risk: Hypoventilation.
Common Modes:
| Mode | Type | Trigger | Cycle | Goal | Pro | Con |
|---|---|---|---|---|---|---|
| AC/CMV | VC/PC | Pt/Time | Vol/Time | Full support; Set $V_T$/$P_{insp}$ | $V_T$ assured (VC)/$P_{aw}$ limit (PC) | Asynchrony, baro/volutrauma |
| SIMV | VC/PC | Pt/Time (Mand); Pt (Spont) | Vol/Time (Mand); Flow (Spont) | Weaning, Pt sync | ↓Sedation, muscle use | ↑WOB if low |
| PSV | Pressure | Pt | Flow | Spont. support, weaning | Comfort, ↓WOB | Apnea risk, variable $V_T$ |
| PRVC | Hybrid | Pt/Time | Time | Target $V_T$ @ low $P_{aw}$ | $V_T$ assured, $P_{aw}$ protected | Slow response |
| %%{init: {'flowchart': {'htmlLabels': true}}}%% | ||||||
| flowchart TD |
FullControl["💨 Full Control
• AC/CMV mode• VC and PC modes"]
PartialSupport["🌬️ Partial Support
• SIMV plus PSV• Patient efforts"]
Spontaneous["🫁 Spontaneous
• PSV/CPAP setting• Trialing weaning"]
FullControl -->|Weaning| PartialSupport PartialSupport -->|Transition| Spontaneous
style FullControl fill:#FDF4F3,stroke:#FCE6E4,stroke-width:1.5px,rx:12,ry:12,color:#B91C1C style PartialSupport fill:#FEF8EC,stroke:#FBECCA,stroke-width:1.5px,rx:12,ry:12,color:#854D0E style Spontaneous fill:#F1FCF5,stroke:#BEF4D8,stroke-width:1.5px,rx:12,ry:12,color:#166534
> ⭐ In Pressure Support Ventilation (PSV), cycling from inspiration to expiration typically occurs when inspiratory flow decreases to **25%** of peak inspiratory flow. This is a common default setting.
## Parameters & Monitoring - Fine-Tuning Breaths
* **Key Parameters & Targets:**
- Vt: **6-8** ml/kg IBW (ARDS: **4-6** ml/kg).
- RR: **12-20**/min (target PaCO2).
- FiO2: Start **1.0**, titrate for SpO2 >**92%**.
- PEEP: Start **5** cmH2O, titrate.
- I:E Ratio: **1:2** to **1:3** (longer for obstruction, e.g., **1:4**).
- PIP: <**35-40** cmH2O.
- Pplat: <**30** cmH2O.
> ⭐ Driving Pressure ($P_{plat}$ - PEEP) should be <**15** cmH2O to minimize Ventilator-Induced Lung Injury (VILI).
* **Essential Monitoring:**
- Gas Exchange: ABG, SpO2, EtCO2 (PaCO2-EtCO2 gradient **2-5** mmHg).
- Lung Mechanics:
+ Static Compliance ($C_{L}$): $C_{L} = V_T / (P_{plat} - PEEP)$.
+ Airway Resistance ($R_{aw}$): $R_{aw} = (P_{IP} - P_{plat}) / Flow$.
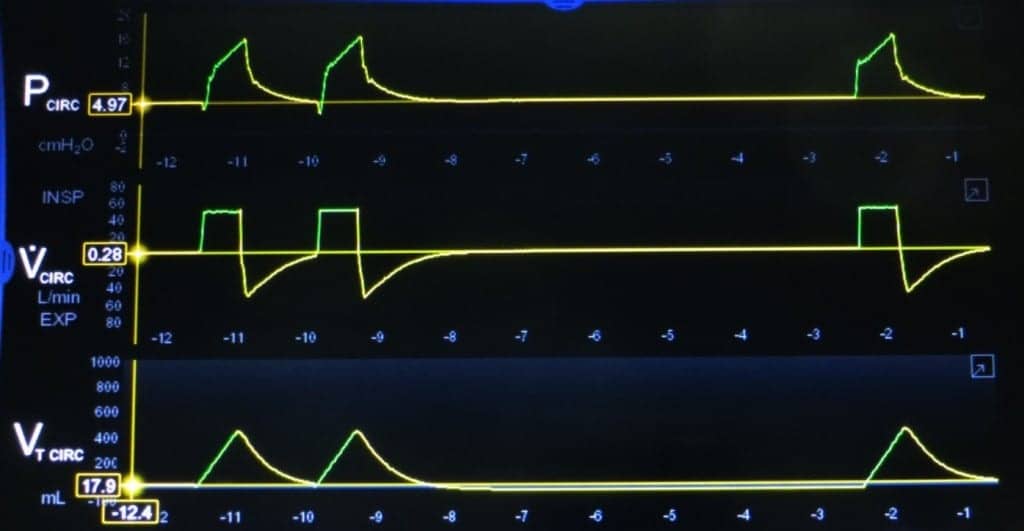
- Waveforms: Crucial for detecting asynchrony, auto-PEEP, leaks.
## Complications & Weaning - Escape from the Machine
**Complications:**
* Ventilator-Associated Pneumonia (VAP):
- Prevention: 📌 **HOST** bundle (**H**OB elevation **30-45°**, **O**ral care, **S**ubglottic suction, **T**rials of spontaneous breathing).
* Barotrauma/Volutrauma: Pneumothorax risk; monitor peak/plateau pressures.
* Oxygen Toxicity: From prolonged FiO2 > **0.6**; aim SpO2 **92-96%**.
* Cardiovascular: ↓Preload, hypotension from ↑intrathoracic pressure.
* Auto-PEEP: Air trapping, ↑work of breathing.
**Weaning:**
* Criteria: Improved underlying cause, stable hemodynamics, PaO2/FiO2 > **150-200**, PEEP ≤ **5-8** cmH2O, FiO2 ≤ **0.4**. Good cough. RSBI < **105** ($RSBI = RR / V_T$ in Liters).
* Spontaneous Breathing Trial (SBT): **30-120** min on T-piece or low Pressure Support Ventilation (PSV).
* Common Weaning Modes: PSV, T-piece trial.
```mermaid
%%{init: {'flowchart': {'htmlLabels': true}}}%%
flowchart TD
Start["<b>🫁 MV Patient</b><br><span style='display:block; text-align:left; color:#555'>• Mech ventilation</span><span style='display:block; text-align:left; color:#555'>• ICU admission</span>"]
Assess["<b>📋 Ready to Wean?</b><br><span style='display:block; text-align:left; color:#555'>• Assess criteria</span><span style='display:block; text-align:left; color:#555'>• Clinical screen</span>"]
ContinueMV["<b>👁️ Continue MV</b><br><span style='display:block; text-align:left; color:#555'>• Optimize support</span><span style='display:block; text-align:left; color:#555'>• Ongoing care</span>"]
RSBI["<b>📋 RSBI < 105?</b><br><span style='display:block; text-align:left; color:#555'>• Rapid shallow breathing</span><span style='display:block; text-align:left; color:#555'>• f/Vt ratio check</span>"]
SBT["<b>🔬 SBT</b><br><span style='display:block; text-align:left; color:#555'>• Spontaneous breath</span><span style='display:block; text-align:left; color:#555'>• Trial period</span>"]
Resume["<b>👁️ Resume Support</b><br><span style='display:block; text-align:left; color:#555'>• Resume settings</span><span style='display:block; text-align:left; color:#555'>• Further optimize</span>"]
Extubate["<b>💊 Extubate</b><br><span style='display:block; text-align:left; color:#555'>• Remove tube</span><span style='display:block; text-align:left; color:#555'>• Monitor airway</span>"]
Start --> Assess
Assess -->|Not Ready| ContinueMV
Assess -->|Criteria Met| RSBI
RSBI -->|Yes| SBT
RSBI -->|RSBI High| Resume
SBT -->|Tolerated| Extubate
SBT -->|Failed| Resume
style Start fill:#F7F5FD, stroke:#F0EDFA, stroke-width:1.5px, rx:12, ry:12, color:#6B21A8
style Assess fill:#FEF8EC, stroke:#FBECCA, stroke-width:1.5px, rx:12, ry:12, color:#854D0E
style ContinueMV fill:#EEFAFF, stroke:#DAF3FF, stroke-width:1.5px, rx:12, ry:12, color:#0369A1
style RSBI fill:#FEF8EC, stroke:#FBECCA, stroke-width:1.5px, rx:12, ry:12, color:#854D0E
style SBT fill:#FFF7ED, stroke:#FFEED5, stroke-width:1.5px, rx:12, ry:12, color:#C2410C
style Resume fill:#EEFAFF, stroke:#DAF3FF, stroke-width:1.5px, rx:12, ry:12, color:#0369A1
style Extubate fill:#F1FCF5, stroke:#BEF4D8, stroke-width:1.5px, rx:12, ry:12, color:#166534
⭐ The Rapid Shallow Breathing Index (RSBI) is a critical predictor for weaning success; a value < 105 indicates a high likelihood of successful extubation.
High‑Yield Points - ⚡ Biggest Takeaways
- Tidal Volume (Vt): Target 6-8 mL/kg PBW, especially in ARDS, for lung protection.
- PEEP: Optimizes oxygenation and prevents alveolar collapse; titrate for best compliance.
- Plateau Pressure (Pplat): Keep <30 cmH2O to minimize barotrauma/volutrauma.
- Driving Pressure (ΔP): Aim for <15 cmH2O (Pplat - PEEP), critical in ARDS.
- Modes: Know ACVC, ACPC, SIMV, PSV indications and differences.
- Weaning: Daily Spontaneous Breathing Trials (SBT) are crucial for liberation from ventilation.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more