USMLE Step 2 CK Psychiatry: High-Yield Topics, DSM-5 Criteria and Question Strategy (2026)
Master psychiatry for USMLE Step 2 CK with high-yield topics, DSM-5 criteria breakdowns, antipsychotic pharmacology, and question strategies that boost your score.
USMLE Step 2 CK Psychiatry: High-Yield Topics, DSM-5 Criteria and Question Strategy (2026)
You are probably staring at your Step 2 CK prep schedule right now, wondering if you can really master psychiatry in the time you have left. Here's what most students dont realize: psychiatry makes up 10-15% of Step 2 CK — thats roughly 32-48 questions on your exam. Yet its the block most students under-prepare for, thinking they can wing it with basic knowledge from their psych rotation.
The reality? Psychiatry questions on Step 2 CK are precision instruments. They test exact DSM-5 duration thresholds, symptom counts, and exclusion criteria. The difference between major depressive disorder and dysthymia isnt just severity — its the 2-week versus 2-year timeline. The difference between schizophrenia and brief psychotic disorder? Six months versus one month total duration.
You cant afford to guess. When a vignette gives you a patient with "5 months of auditory hallucinations and delusions that resolved completely after treatment," thats schizophreniform disorder — not schizophrenia, not brief psychotic disorder. The exam rewards students who know these distinctions cold.
This guide breaks down the highest-yield psychiatry topics for Step 2 CK, shows you how DSM-5 criteria map to exam vignettes, and gives you a systematic approach to psychiatric questions that will save you time and boost your score.
High-Yield Psychiatry Topics for Step 2 CK
Mood Disorders: The Duration Game
Mood disorders are the heaviest hitters in psychiatry — expect 8-12 questions just in this category. The key insight: Step 2 CK loves testing the boundaries between similar conditions.
Major Depressive Disorder (MDD) requires 5 out of 9 SIG E CAPS criteria for at least 2 weeks: Sleep changes, Interest loss, Guilt/worthlessness, Energy loss, Concentration problems, Appetite changes, Psychomotor changes, Suicidal ideation. Remember: the episode must cause significant functional impairment. Persistent Depressive Disorder (Dysthymia) is the 2-year version — depressed mood more days than not for 2+ years, with 2+ additional symptoms, but never meeting full MDD criteria during the first 2 years. Bipolar I requires just ONE lifetime manic episode (1+ weeks or hospitalization required). A major depressive episode can occur in bipolar I — the question is whether there has EVER been mania. Bipolar II requires at least one hypomanic episode (4+ days) plus at least one major depressive episode, but NEVER a full manic episode. Cyclothymia is 2+ years of cycling between hypomanic symptoms and depressive symptoms without ever meeting full criteria for either a manic, hypomanic, or major depressive episode.
The exam trick: when you see mood symptoms, immediately scan for prior episode history. If theres ANY mention of past mania or hypomania, MDD is off the table.
Practice these distinctions with mood disorder MCQs that test these exact boundaries.
Psychotic Disorders: Timeline is Everything
Schizophrenia requires 6+ months of continuous signs (including prodromal or residual periods) with at least 1 month of active psychosis (delusions, hallucinations, or disorganized speech). Functional decline is required. Schizophreniform Disorder is exactly like schizophrenia but lasts 1-6 months total. Brief Psychotic Disorder lasts at least 1 day but less than 1 month, with eventual return to normal functioning. Schizoaffective Disorder requires mood episodes (major depression or mania) concurrent with psychotic symptoms for the majority of the illness duration, PLUS at least 2 weeks of psychosis without prominent mood symptoms. Delusional Disorder involves fixed false beliefs for 1+ months without other significant psychotic symptoms, and functioning remains relatively intact except for the delusion's impact.
The vignette pattern: look for duration cues first, then functional impairment level. A patient who "had 3 weeks of hearing voices but returned to work normally" is brief psychotic disorder, not schizophrenia.
Anxiety Disorders: Know Your Timelines
Generalized Anxiety Disorder (GAD) requires excessive worry about multiple life events for 6+ months, difficult to control, with 3+ physical symptoms (restlessness, fatigue, concentration problems, irritability, muscle tension, sleep disturbance). Panic Disorder requires recurrent unexpected panic attacks plus 1+ months of persistent concern about additional attacks or maladaptive behavior changes. The attacks peak within minutes and include 4+ symptoms: palpitations, sweating, trembling, shortness of breath, choking sensation, chest pain, nausea, dizziness, derealization, fear of losing control, fear of dying, numbness, hot/cold flashes. PTSD requires exposure to trauma (direct, witness, learn about close person, or repeated professional exposure) plus 1+ symptoms from each cluster for 1+ months: intrusive memories, avoidance, negative mood/cognition changes, arousal/reactivity changes. Social Anxiety Disorder involves marked fear of social situations where scrutiny might occur, lasting 6+ months with functional impairment.
Personality Disorders: Cluster B Dominates
Step 2 CK focuses heavily on Cluster B personality disorders:
Borderline Personality Disorder: unstable relationships, identity disturbance, impulsivity, recurrent suicidal behavior, affective instability, chronic emptiness, inappropriate anger, paranoid ideation under stress. Antisocial Personality Disorder: pattern of violating others rights since age 15, with conduct disorder evidence before age 15. Look for deceitfulness, impulsivity, irritability, reckless disregard for safety, irresponsibility, lack of remorse. Narcissistic and Histrionic appear less frequently but know the core features: grandiosity + lack of empathy for narcissistic; attention-seeking + emotional dysregulation for histrionic.
Substance Use Disorders: Withdrawal Timelines
Know the withdrawal timelines and treatment protocols:
Alcohol withdrawal: symptoms start 6-12 hours after last drink, peak 24-48 hours. Treat with benzodiazepines (chlordiazepoxide, lorazepam). Watch for delirium tremens at 48-72 hours. Opioid withdrawal: starts 6-12 hours (short-acting) to 1-3 days (long-acting), peaks 1-3 days. Treat with buprenorphine, methadone, or clonidine for symptom management. Benzodiazepine withdrawal: can be life-threatening. Taper slowly over weeks to months depending on half-life. Stimulant withdrawal: primarily psychological — depression, fatigue, vivid dreams, increased appetite, psychomotor changes.
Refresh these concepts with targeted psychiatry flashcards for active recall practice.
How DSM-5 Maps to Exam Vignettes
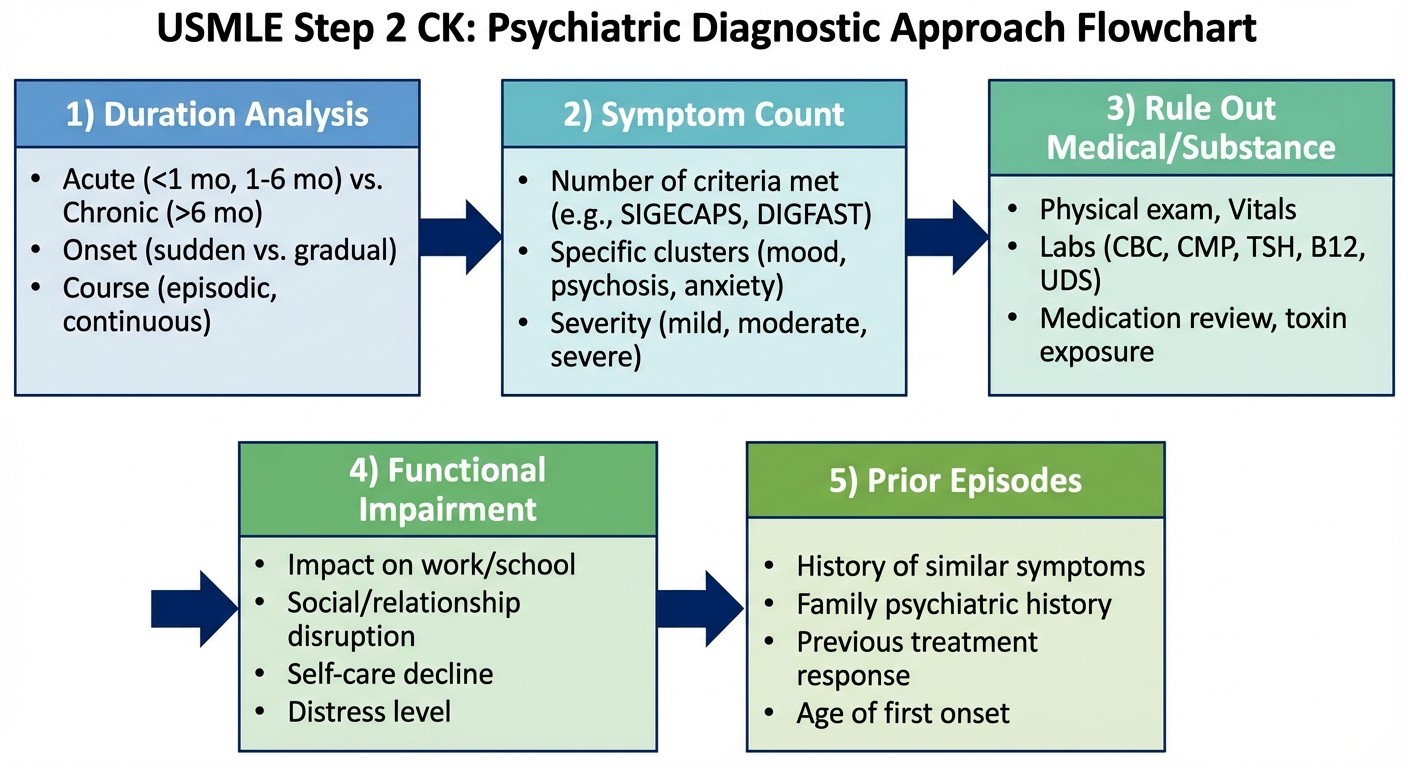
Step 2 CK vignettes follow a predictable pattern that mirrors real clinical assessment. Heres your systematic approach:
Step 1: Duration and Timeline Analysis
Always read for time indicators first. The exam plants these deliberately:
"Over the past 3 weeks..." (Brief psychotic disorder territory)
"For the last 8 months..." (Schizophrenia possible)
"Since childhood..." (Personality disorder or developmental)
"Every winter for 3 years..." (Seasonal pattern)
Step 2: Count Symptoms Precisely
DSM-5 requires specific symptom thresholds. When you see mood symptoms, count the SIG E CAPS criteria explicitly. When you see psychotic symptoms, identify which of the 5 categories are present (delusions, hallucinations, disorganized speech, grossly disorganized behavior, negative symptoms).
For example: if a vignette lists "poor sleep, loss of appetite, difficulty concentrating, feelings of guilt, and loss of interest in activities for 3 weeks," thats 5 out of 9 SIG E CAPS criteria for 3+ weeks — meets MDD threshold.
Step 3: Rule Out Medical and Substance Causes
The exam expects you to consider organic causes before making psychiatric diagnoses. Look for:
Substance use history (always ask about alcohol, illicit drugs, medications)
Medical conditions (thyroid disease, vitamin deficiencies, neurological conditions)
Medication side effects
If the vignette mentions "recent cocaine use" or "started on steroids 2 weeks ago," consider substance-induced mood disorder before primary psychiatric conditions.
Step 4: Assess Functional Impairment
DSM-5 requires significant distress or functional impairment for most diagnoses. The exam tests this by describing work performance, relationships, or daily activities. "Missed 2 weeks of work" signals functional impairment. "Maintains excellent job performance" might point toward adjustment disorder rather than major mental illness.
Step 5: Prior Episode History
This is crucial for mood disorders. If theres ANY history of mania or hypomania, current depression is part of bipolar disorder, not unipolar depression. The exam might bury this in the history: "had a period in college where she needed little sleep, was very energetic, and made impulsive decisions" — thats a hypomanic episode.
Antipsychotic and Mood Stabilizer Pharmacology
Pharmacology questions are high-yield and follow predictable patterns. Know the side effect profiles cold:
First-Generation (Typical) Antipsychotics
Haloperidol is the prototype. High potency = high extrapyramidal symptoms (EPS) risk. Watch for acute dystonia, akathisia, parkinsonism, and tardive dyskinesia. Also carries neuroleptic malignant syndrome (NMS) risk. Chlorpromazine is low potency = more anticholinergic and sedating effects, less EPS.
Second-Generation (Atypical) Antipsychotics
Each has a signature side effect profile:
Clozapine: agranulocytosis (requires weekly CBC monitoring for 6 months, then biweekly), seizures, significant metabolic effects (weight gain, diabetes, dyslipidemia). Reserved for treatment-resistant schizophrenia. Olanzapine: highest metabolic risk among atypicals — significant weight gain, diabetes, dyslipidemia. Effective but monitor metabolically. Risperidone: highest EPS risk among atypicals, significant hyperprolactinemia (gynecomastia, galactorrhea, amenorrhea). Quetiapine: very sedating, metabolic effects, but lowest prolactin elevation. Good for bipolar depression. Ziprasidone: QTc prolongation risk — get baseline EKG and monitor. Least metabolic effects. Aripiprazole: partial dopamine agonist, so less metabolic effects and prolactin elevation, but can cause significant akathisia. "Activating" rather than sedating.
Mood Stabilizers
Lithium: narrow therapeutic window (0.6-1.2 mEq/L). Toxicity signs: tremor, confusion, seizures, coma. Monitor kidney function, thyroid function. Can cause diabetes insipidus. Valproate: teratogenic (neural tube defects) — contraindicated in pregnancy. Monitor liver function, CBC (thrombocytopenia risk). Good for rapid cycling bipolar. Carbamazepine: potent P450 inducer — multiple drug interactions. Monitor CBC (agranulocytosis risk), liver function. Can cause hyponatremia. Lamotrigine: major concern is Stevens-Johnson syndrome with rapid titration. Start low, titrate slowly. Good for bipolar depression.
The exam pattern: they give you a side effect and ask for the most likely medication, or give you a medication and ask about monitoring requirements. When you practice psychiatry assessment questions, focus on these medication-outcome pairs.
Question Strategy for the Psychiatry Block
Safety First, Always
Every psychiatric encounter starts with safety assessment. If the vignette mentions suicidal ideation, your first step is assessing plan, intent, and means — not starting antidepressants. Active suicidal ideation with plan and means requires immediate hospitalization.
Similarly, homicidal ideation requires immediate assessment and potentially breaking confidentiality (duty to warn). Violence risk factors include: command hallucinations, paranoid delusions about specific people, substance use, antisocial personality disorder.
Most Appropriate NEXT Step Questions
These are classic Step 2 CK format. The answer is often NOT the ultimate treatment, but the most appropriate immediate action:
Establish rapport first: "validate the patient's concerns" often beats "start medication"
Assess before treating: "obtain collateral history from family" before diagnosing
Rule out organic causes: "check TSH and B12" before antidepressants for new-onset depression in elderly patients
Safety assessment: "assess suicidal ideation" before discharge planning
Hospitalization Criteria
Know when inpatient treatment is required:
Active suicidal ideation with plan, intent, or means
Active homicidal ideation
Inability to care for self due to psychiatric symptoms
Psychosis with poor insight and dangerous behavior
Severe substance withdrawal requiring medical monitoring
Outpatient treatment is appropriate for stable patients with good social support, insight into illness, and no immediate safety concerns. When you encounter clinical scenarios in psychiatry, practice these safety assessments systematically.
Therapeutic Approach Questions
The exam tests your knowledge of evidence-based treatments:
First-line treatments to know:
MDD: SSRIs (sertraline, escitalopram) + psychotherapy
GAD: SSRIs or SNRIs + CBT
Panic disorder: SSRIs + CBT
PTSD: trauma-focused psychotherapy + SSRIs
OCD: high-dose SSRIs + exposure and response prevention therapy
Bipolar I acute mania: mood stabilizer + antipsychotic
Schizophrenia: antipsychotic + psychosocial rehabilitation
Second-line considerations:
Treatment-resistant depression: switch SSRI class, add bupropion, consider TCA or MAOI
Treatment-resistant schizophrenia: clozapine trial
The vignette will usually describe failed first-line treatment to justify second-line options.
Mastering Psychiatry with Targeted Practice
The gap between knowing DSM-5 criteria and applying them under timed conditions is where most students struggle. Passive reading of diagnostic criteria wont cut it — you need active recall practice that mirrors exam conditions.
Oncourses Daily Mnemonic Challenge is a game-based puzzle that uses retrieval practice to lock in critical medical mnemonics. For psychiatry, this is perfect for memorizing the DSM-5 diagnostic criteria that the exam tests with precision. The puzzle format — with letter-by-letter input, a clue card, and only 3 attempts — forces active recall rather than passive re-reading. Working through a mnemonic for SIG E CAPS (MDD criteria) or DIGFAST (manic episode criteria) in a timed, low-stakes puzzle format builds the kind of automatic recall you need when a vignette gives you exactly 5 out of 9 symptoms and you need to count fast. Practice these daily at Oncourse mnemonics.
Pattern recognition across symptom clusters is another critical skill. Oncourses Synapses is a gamified word-grouping challenge that trains exactly this ability. The game presents 4 groups of words (difficulty 1–4) and you have to match them — think: grouping 'flat affect, avolition, alogia, anhedonia' (negative symptoms of schizophrenia) versus 'hallucinations, delusions, disorganized speech' (positive symptoms). The leaderboard mechanics and time-based scoring add competitive stakes that make re-engagement feel natural, so you come back to practice these differentials again and again.
For full clinical reasoning practice, Clinical Rounds simulates the exact 4-step process Step 2 CK tests: History Taking → Order Tests → Diagnosis → Treatment. A psychiatric vignette on Step 2 CK follows this exact structure — the exam gives you a patient history, you have to know which collateral history questions matter (prior manic episodes, family history, substance use), which tests to order (TSH to rule out thyroid, tox screen to rule out substances, B12), make a diagnosis, and then select the right treatment or next step. When you get it wrong, Rezzy AI tutor instantly explains the clinical reasoning that connects the vignette clues to the correct diagnosis and treatment.
Frequently Asked Questions
How much time should I spend on psychiatry for Step 2 CK?
Given that psychiatry comprises 10-15% of the exam, dedicate 1-2 weeks of focused study. Spend 60% of your time on mood and psychotic disorders since these are highest yield, 25% on anxiety and personality disorders, and 15% on substance use and other categories.
What's the most common mistake students make with psychiatry questions?
Not reading for duration and timeline cues first. Students jump to symptom matching without noting that "3 weeks of symptoms" rules out many conditions that require longer duration thresholds.
Do I need to memorize every DSM-5 criterion exactly?
For Step 2 CK, focus on the major disorders and their key distinguishing features: duration requirements, symptom count thresholds, and exclusion criteria. You dont need every personality disorder subtype, but nail the big ones: MDD, bipolar, schizophrenia, GAD, panic disorder.
How detailed should my pharmacology knowledge be?
Know first-line treatments and major side effects. You dont need every drug interaction, but know the signature adverse effects: clozapine and agranulocytosis, olanzapine and metabolic syndrome, lithium and toxicity signs, lamotrigine and rash risk.
What if I cant distinguish between similar conditions in a vignette?
Use the systematic approach: duration first, symptom count second, exclusions third. If youre stuck between schizophrenia and schizoaffective disorder, look for prominence of mood symptoms — schizoaffective has major mood episodes for the majority of the illness.
Should I focus more on diagnosis or treatment questions?
Both are heavily tested, but diagnostic questions tend to be higher yield. Master the differential diagnosis approach first, then layer in treatment knowledge. Many treatment questions become easier when you're confident in the diagnosis.
---
Psychiatry doesnt have to be the section that trips you up on Step 2 CK. With systematic preparation focused on high-yield topics, precise DSM-5 knowledge, and strategic question approach, you can turn this into one of your strongest blocks.
The key insight: treat psychiatric vignettes like diagnostic puzzles with specific rules, not subjective clinical impressions. The exam rewards students who can apply criteria systematically under time pressure.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for USMLE Step 2 CK. Download free on Android and iOS.