
Mood Disorders — MCQs

On this page
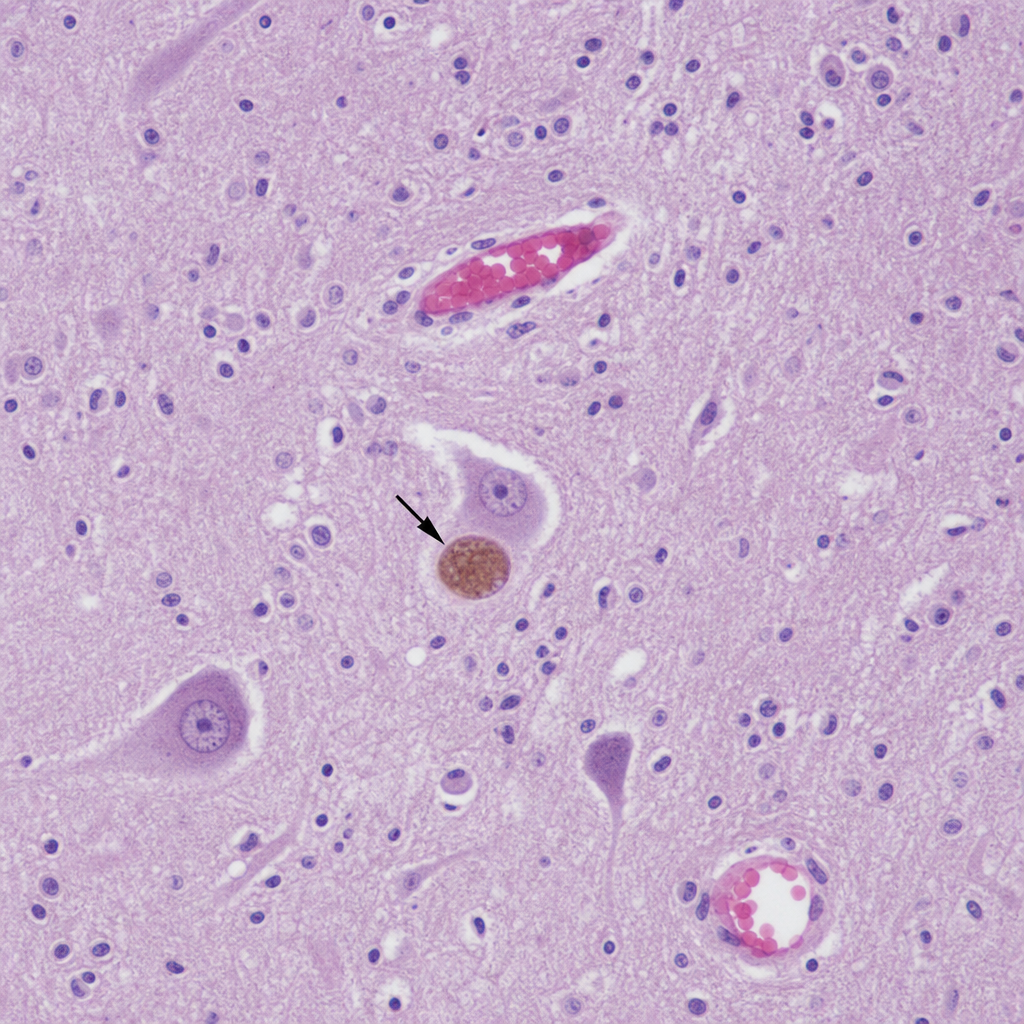
A 58-year-old retired engineer is brought to a memory clinic by his wife, who says he has been getting lost while driving familiar routes for the past 14 months. She also notes he has had two episodes of acting out his dreams violently — he punched the headboard while apparently fighting someone in his sleep. On examination he has mild cogwheel rigidity bilaterally, a resting tremor of the right hand, and a shuffling gait. MMSE is 22/30 with deficits concentrated in visuospatial tasks and attention. Polysomnography demonstrates REM sleep without atonia. Which of the following is the most likely underlying diagnosis?
A 21-year-old woman is brought to the emergency room 1 hour after she ingested 12 pills of acetaminophen. She had a fight with her boyfriend immediately prior to the ingestion, during which she threatened to kill herself if he broke up with her. She has been hospitalized 4 times for overdoses in the past 3 years following breakups with her partners. On the way to the hospital, she screamed and then assaulted the paramedic who attempted to take her temperature. Physical examination shows multiple rows of well-healed scars bilaterally on the wrists. This patient is most likely to display which of the following defense mechanisms?
A 48-year-old man and his wife present to a psychologist's office for a therapy session. He was encouraged to visit the psychiatrist 6 months ago by his wife and they have been meeting with the psychologist several times a month ever since. Initially, she was concerned about behavioral changes she observed after he was passed up for a promotion at work. She felt he was taking on a new personality and was acting like his coworker, who actually did get the promotion. He would also talk about his coworker and praise his intelligence and strategic character. Over the course of several months, the patient bought new clothes that looked like the other man's clothes. He changed his hairstyle and started using phrases that were similar to his coworker. Today, they both seem well. The patient still does not seem to think there is a problem and requests to stop therapy. His wife was frustrated because her husband recently bought a new car of the exact make and model of his coworker. Which of the following defense mechanisms best describes this patient's condition?
A 45-year-old man comes to the physician for a routine health maintenance examination. He is asymptomatic. He reports that he recently found out that his wife had an affair with her personal trainer and that she now left him for her new partner. The patient is alone with their two children now. To be able to care for them, he had to reduce his working hours and to give up playing tennis twice a week. When asked about his feeling towards his wife and the situation, he reports that he has read several books about human emotion recently. He says, “Falling in love has neurological effects similar to those of amphetamines. I suppose, my wife was just seeking stimulation.” Which of the following defense mechanisms best describes this patient's reaction?
A parent-teacher conference is called to discuss the behavior of a 9-year-old boy. According to the boy's teacher, he has become progressively more disruptive during class. He is performing poorly in school and has trouble focusing. He is destructive to classroom property, tore a classmate's art project, and takes other children's lunches regularly. He is avoided by his classmates. His mother reports that her son can "sometimes be difficult." Recently he placed a rubber band around the cats tail, resulting in gangrene. What is the most likely diagnosis?
Practice by Chapter
Persistent depressive disorder (dysthymia)
Practice Questions
Premenstrual dysphoric disorder
Practice Questions
Disruptive mood dysregulation disorder
Practice Questions
Adjustment disorder with depressed mood
Practice Questions
Substance-induced mood disorders
Practice Questions
Mood disorders due to medical conditions
Practice Questions
Bereavement and complicated grief
Practice Questions
Mood disorder epidemiology
Practice Questions
Cultural aspects of mood disorders
Practice Questions
Child and adolescent mood disorders
Practice Questions
Geriatric mood disorders
Practice Questions
Comorbidities with mood disorders
Practice Questions
Functional impairment assessment
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app