Back
USMLE Step 2 CK Nephrology: High-Yield Topics, Clinical Vignette Strategy and Exam Checklist (2026)
Master USMLE Step 2 CK nephrology with high-yield topics, clinical vignette strategy, and exam checklist. AKI, CKD, electrolytes, glomerulonephritis, and more.

USMLE Step 2 CK Nephrology: High-Yield Topics, Clinical Vignette Strategy and Exam Checklist (2026)
You're 8 weeks out from Step 2 CK and nephrology vignettes still make your head spin. A 67-year-old man presents with acute kidney injury, muddy brown casts, and a FENa of 2.1% — is this prerenal or intrinsic? The clock's ticking, you have 63 seconds per question, and getting this wrong cascades into missing the next 3 nephrology questions.
Here's the thing: Step 2 CK nephrology isn't about memorizing pathophysiology pathways anymore. It's pure clinical decision-making. Can you distinguish nephrotic from nephritic in 15 seconds? Do you know when to order a renal biopsy versus starting ACE inhibitors? Can you decode the electrolyte panel that screams "RTA Type 1" before reading the rest of the vignette?
This guide breaks down every high-yield nephrology domain that shows up on Step 2 CK, gives you a 60-second vignette strategy, and ends with a checklist you can use 48 hours before test day. No fluff, just the clinical patterns that separate 260+ scorers from everyone else.
How Step 2 CK Tests Nephrology Differently
Step 1 tested nephrology physiology — sodium reabsorption sites, countercurrent mechanisms, renin-angiotensin cascades. Step 2 CK tests nephrology management. Every vignette presents a clinical scenario where you must choose the next best step, interpret lab values in context, or select appropriate treatment.
The shift is fundamental. Instead of "What transporter is defective in Gitelman syndrome?", Step 2 CK asks "A 28-year-old woman presents with muscle cramps, hypokalemia, and hypomagnesemia. What is the most appropriate initial treatment?" The pathophysiology knowledge helps, but clinical judgment wins.
Classic CK-style nephrology traps:
FENa calculations in CKD patients (unreliable when baseline creatinine >2.5)
Confusing nephrotic syndrome features (heavy proteinuria) with nephritic features (hematuria, HTN)
Missing RTA clues buried in normal-looking electrolyte panels
Ordering renal biopsy when clinical diagnosis is clear
Starting dialysis too early or too late
Acute Kidney Injury (AKI): The 3-Category Framework
AKI appears on 15-20% of nephrology questions. Step 2 CK loves testing the prerenal/intrinsic/postrenal distinction because it drives management decisions immediately.
Prerenal AKI (60% of cases)
Clinical picture: Volume depletion, hypotension, heart failure, NSAIDs, ACE inhibitors Lab pattern: BUN:Cr ratio >20:1, FENa <1%, FEUrea <35% Urine: No casts or only hyaline casts Management: Fluid resuscitation, stop offending drugs, treat underlying cause Step 2 CK pearl: FENa <1% strongly suggests prerenal AKI, but this fails in patients on diuretics (use FEUrea instead) or with baseline CKD. Oncourse's nephrology question bank drills these FENa interpretation scenarios — after each answer, AI-powered explanations walk through the clinical reasoning for why specific cutoffs work or fail in different clinical contexts.
Intrinsic AKI (35% of cases)
Acute tubular necrosis (ATN): Most common intrinsic cause
Ischemic ATN: Prolonged hypotension, surgery, sepsis
Nephrotoxic ATN: Aminoglycosides, contrast, myoglobin, hemoglobin
Lab pattern: BUN:Cr ratio 10-15:1, FENa >2%, FEUrea >50% Urine: Muddy brown casts (pathognomonic for ATN), epithelial cells Management: Supportive care, avoid nephrotoxins, optimize hemodynamics Glomerulonephritis: Covered in detail below Acute interstitial nephritis: NSAIDs, antibiotics, PPIs
Urine: Eosinophils, WBC casts
Treatment: Stop offending drug, consider steroids
Postrenal AKI (5% of cases)
Causes: Stones, BPH, tumors, retroperitoneal fibrosis Diagnosis: Hydronephrosis on ultrasound, elevated post-void residual Management: Relieve obstruction (catheter, nephrostomy, ureteral stents)
Chronic Kidney Disease (CKD): Staging and Complications
CKD staging questions are Step 2 CK favorites because they test both classification knowledge and management decisions at each stage.
Stage | GFR (mL/min/1.73m²) | Key Management |
|---|---|---|
1 | ≥90 + kidney damage | ACE/ARB, diabetes control |
2 | 60-89 + kidney damage | Screen for complications |
3a | 45-59 | Nephrology referral |
3b | 30-44 | Bone disease screening |
4 | 15-29 | Prepare for RRT |
5 | <15 or dialysis | Start RRT |
CKD complications by stage:
Stage 3: Anemia (EPO deficiency), bone disease (↓1,25-dihydroxy vitamin D)
Stage 4: Metabolic acidosis, hyperphosphatemia, secondary hyperparathyroidism
Stage 5: Uremia, fluid overload, severe electrolyte abnormalities
Management pearls:
ACE/ARB for proteinuria >30mg/g (even with normal GFR)
Target BP <130/80 in CKD
Avoid contrast when GFR <30 unless dialysis planned
Pneumococcal and hepatitis B vaccines before stage 5
Electrolyte Disorders: The High-Yield Patterns
Electrolyte questions test pattern recognition and acute management. Know the classic presentations cold.
Hyponatremia
Hypovolemic: Diuretics, GI losses, adrenal insufficiency
Treatment: Normal saline
Euvolemic: SIADH, hypothyroidism, psychogenic polydipsia
Treatment: Fluid restriction, salt tablets
Hypervolemic: Heart failure, cirrhosis, nephrotic syndrome
Treatment: Diuretics, treat underlying condition
Correction rate: 0.5-1 mEq/L/hour (max 10-12 mEq/L in 24 hours) to avoid central pontine myelinolysis
Hypernatremia
Always indicates free water deficit Hypovolemic: GI losses, diuretics, osmotic diuresis Euvolemic: Diabetes insipidus (central or nephrogenic) Hypervolemic: Mineralocorticoid excess, hypertonic saline Treatment: Free water replacement, correct slowly (0.5 mEq/L/hour)
Hypokalemia
Causes: Diuretics, hyperaldosteronism, GI losses, poor intake Symptoms: Muscle weakness, paralysis, arrhythmias Treatment: Oral KCl (preferred), IV KCl if severe (<2.5 mEq/L)
Hyperkalemia
Causes: ACE/ARB, K-sparing diuretics, CKD, acidosis ECG changes: Peaked T waves → PR prolongation → wide QRS → sine wave Treatment: 1. Acute: Calcium gluconate (cardioprotective) 2. Shift K+ intracellularly: Insulin + glucose, albuterol, bicarb 3. Remove K+: Kayexalate, diuretics, dialysis
The mnemonic "Some Patients Take Kayexalate" covers hyperkalemia treatment: Stabilize (calcium), Push inside (insulin/glucose), Take it out (Kayexalate). Oncourse's spaced repetition flashcards surface these electrolyte patterns at scientifically optimized intervals — you review each card just before you'd forget it, locking in the clinical vignette traps that appear on Step 2 CK.
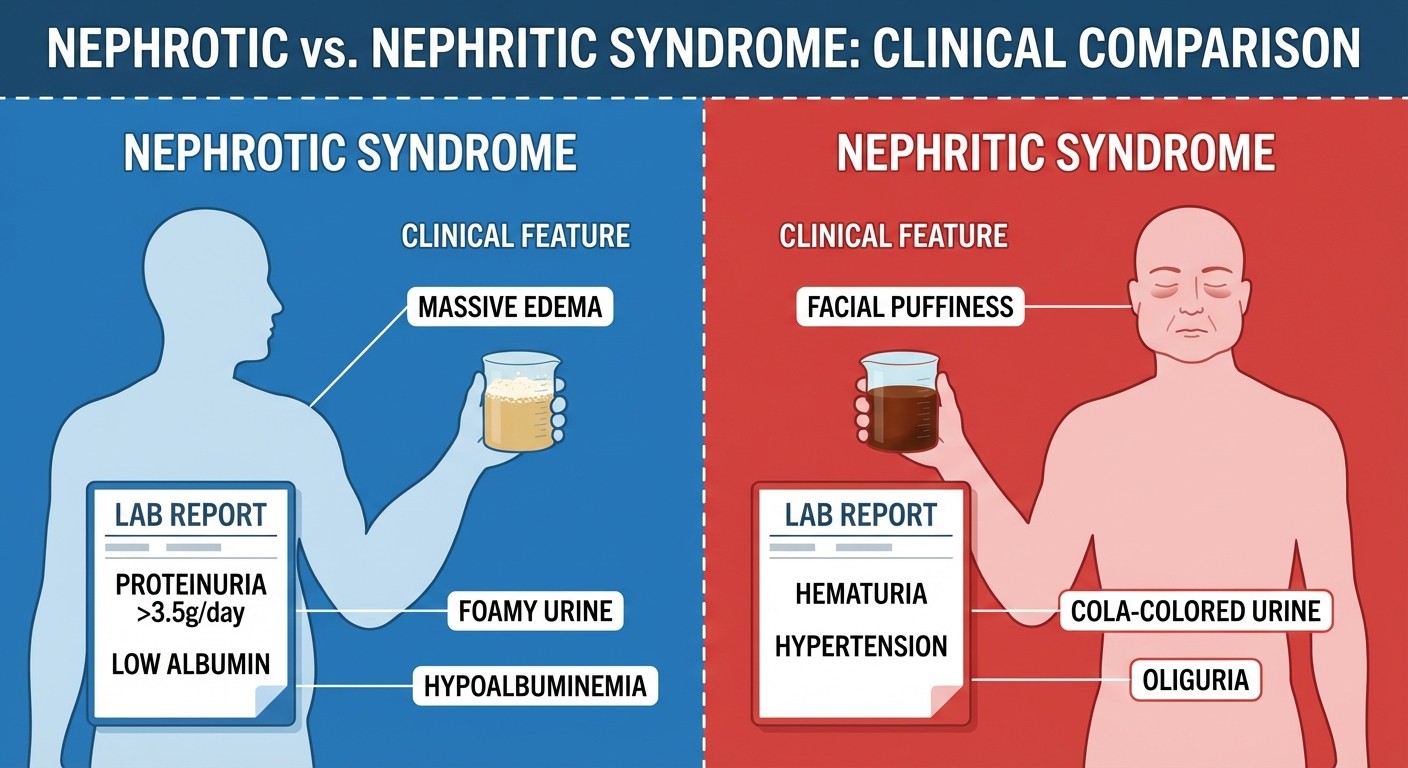
Glomerulonephritis: Nephrotic vs Nephritic
This is where Step 2 CK separates students who memorized lists from those who understand clinical patterns. The key is recognizing whether proteinuria or hematuria dominates the presentation.
Nephrotic Syndrome
Definition: Proteinuria >3.5g/day, hypoalbuminemia, edema, hyperlipidemia Classic presentation: Gradual onset, massive edema, foamy urine
Disease | Age Group | Key Features | Treatment |
|---|---|---|---|
MCD | Children | Responds to steroids | Prednisone |
FSGS | Young adults | HTN, progressive | ACE/ARB, steroids |
Membranous | Older adults | Hepatitis B, cancer association | Supportive care |
Diabetic nephropathy | Diabetes | Most common overall | ACE/ARB, glucose control |
Nephritic Syndrome
Definition: Hematuria, HTN, edema, proteinuria <3g/day Classic presentation: Acute onset, "coca-cola" urine, facial puffiness
Disease | Timing | Key Features | Treatment |
|---|---|---|---|
Post-strep GN | 1-2 weeks post-infection | Low C3, ASO titers | Supportive |
IgA nephropathy | Days after URI | Most common GN worldwide | ACE/ARB |
RPGN | Days to weeks | Crescents on biopsy, ANCA | Steroids, cyclophosphamide |
Step 2 CK pearl: If proteinuria >3.5g/day, think nephrotic first. If hematuria + HTN + acute onset, think nephritic. Don't get trapped by mixed presentations — diabetic nephropathy can have hematuria, FSGS can have HTN.
Renal Tubular Acidosis (RTA): The Pattern Recognition Game
RTA questions test your ability to match clinical patterns with specific defects. Each type has a signature lab pattern.
Type 1 (Distal) RTA
Defect: Cannot acidify urine (urine pH >5.5) Lab pattern: Normal anion gap metabolic acidosis, hypokalemia, hypercalciuria Complications: Nephrolithiasis (calcium phosphate stones), nephrocalcinosis Causes: Autoimmune diseases, hypergammaglobulinemia
Type 2 (Proximal) RTA
Defect: Cannot reabsorb bicarbonate Lab pattern: Normal anion gap metabolic acidosis, hypokalemia when treated Complications: Growth retardation, rickets Causes: Fanconi syndrome, carbonic anhydrase inhibitors
Type 4 RTA
Defect: Aldosterone deficiency or resistance Lab pattern: Normal anion gap metabolic acidosis, hyperkalemia Causes: Diabetes, NSAIDs, ACE inhibitors, K-sparing diuretics Memory trick: Type 1 = kidney stones (distal tubule can't make acid), Type 2 = bicarbonate wasting (proximal), Type 4 = high potassium (aldosterone problem).
Nephrolithiasis: Stone Types and Management
Stone composition drives both acute management and prevention strategies.
Stone Types by Frequency
1. Calcium oxalate (80%): Radiopaque, associated with hypercalciuria, low citrate 2. Calcium phosphate (15%): Radiopaque, alkaline urine, RTA Type 1 3. Uric acid (5%): Radiolucent, acidic urine, gout, high purine diet 4. Struvite (<5%): Radiopaque, alkaline urine, urease-producing bacteria 5. Cystine (rare): Hereditary, hexagonal crystals
Acute Management
<5mm stones: Supportive care, hydration, pain control 5-10mm stones: Medical expulsion therapy (tamsulosin) >10mm stones: Lithotripsy or ureteroscopy Prevention by stone type:
Calcium stones: Thiazides (↓ calciuria), citrate supplementation
Uric acid stones: Allopurinol, alkalinize urine
Struvite stones: Treat infection, complete stone removal
Hypertension and Renal Disease
HTN both causes and complicates kidney disease. Step 2 CK tests the bidirectional relationship.
Secondary HTN causes (renal):
Renovascular disease: Renal artery stenosis (especially in young women or older men with atherosclerosis)
Primary aldosteronism: HTN + hypokalemia + metabolic alkalosis
Pheochromocytoma: Episodic HTN + headaches + sweating
HTN management in CKD:
Goal: <130/80 mmHg
First-line: ACE/ARB (especially with proteinuria)
Add: Thiazides, calcium channel blockers
Avoid: K-sparing diuretics if GFR <30
Dialysis Indications: The AEIOU Mnemonic
Know when to start renal replacement therapy (RRT). The AEIOU mnemonic covers absolute indications:
Acidosis (severe metabolic acidosis, pH <7.1)
Electrolytes (hyperkalemia >6.5 mEq/L, refractory)
Intoxications (methanol, ethylene glycol, lithium)
Overload (pulmonary edema, refractory to diuretics)
Uremia (pericarditis, encephalopathy, bleeding)
Relative indications:
GFR <10-15 mL/min/1.73m² with uremic symptoms
Progressive decline despite optimal medical management
Clinical Vignette Strategy: Decode in 60 Seconds
Step 2 CK nephrology vignettes follow predictable patterns. Here's how to decode them systematically:
First 15 seconds: Pattern Recognition
Scan for these key phrases:
"Acute onset" + oliguria = AKI
"Foamy urine" + edema = nephrotic syndrome
"Dark urine" + HTN = nephritic syndrome
"Muscle weakness" + K+ abnormality = electrolyte disorder
Next 15 seconds: Lab Analysis
Check these values in order: 1. Creatinine: Normal (0.6-1.2) vs elevated (AKI vs CKD) 2. Proteinuria: <3g/day (nephritic) vs >3.5g/day (nephrotic) 3. Electrolytes: Focus on Na+, K+, CO2 (bicarb) 4. Urinalysis: Casts (muddy brown = ATN), crystals, cells
Next 15 seconds: Clinical Context
Age and comorbidities matter:
Elderly + heart failure = prerenal AKI likely
Young + recent URI = post-infectious GN
Diabetes + proteinuria = diabetic nephropathy
Autoimmune disease = lupus nephritis
Final 15 seconds: Choose Management
Step 2 CK tests next best step, not diagnosis:
AKI: Fluid challenge vs stop nephrotoxins vs imaging
Electrolyte disorder: Acute treatment vs long-term management
GN: Supportive care vs biopsy vs immunosuppression
Oncourse's AI engine analyzes your performance across nephrology sub-topics and schedules targeted review sessions. If you keep getting AKI management questions wrong, the daily adaptive study plan front-loads those scenarios before moving to electrolyte or glomerulonephritis topics — particularly useful in the Step 2 CK push phase when time is scarce.
USMLE Step 2 CK Nephrology Exam Checklist
Use this checklist 48 hours before test day. If you can confidently check off each item, you're ready for nephrology questions.
AKI and CKD
[ ] Can distinguish prerenal/intrinsic/postrenal AKI in 30 seconds
[ ] Know FENa cutoffs and when they fail (diuretics, CKD)
[ ] Remember muddy brown casts = ATN
[ ] Can stage CKD and know complications by stage
[ ] Know when to refer to nephrology (GFR <45)
Electrolyte Disorders
[ ] Can classify hyponatremia by volume status
[ ] Know hyperkalemia ECG changes and treatment sequence
[ ] Remember hyponatremia correction rate (10-12 mEq/L max per day)
[ ] Can distinguish central vs nephrogenic diabetes insipidus
Glomerulonephritis
[ ] Can differentiate nephrotic vs nephritic syndrome instantly
[ ] Know which GN diseases affect which age groups
[ ] Remember MCD responds to steroids, FSGS doesn't
[ ] Know post-strep GN timing (1-2 weeks post-infection)
RTA and Acid-Base
[ ] Can match RTA type to lab pattern (K+ levels, urine pH)
[ ] Know Type 1 causes kidney stones, Type 4 causes hyperkalemia
[ ] Can calculate anion gap and classify metabolic acidosis
Stones and HTN
[ ] Know stone types by radiopacity and urine pH
[ ] Remember thiazides prevent calcium stones
[ ] Know secondary HTN workup triggers
[ ] Can list AEIOU dialysis indications
Management Decisions
[ ] Know when to start ACE/ARB (proteinuria >30mg/g)
[ ] Can choose between renal ultrasound vs CT vs biopsy
[ ] Know when dialysis is emergent vs elective
[ ] Remember BP goal in CKD (<130/80)
Frequently Asked Questions
How much of Step 2 CK is nephrology?
Nephrology comprises roughly 8-12% of Step 2 CK questions, translating to 25-35 questions on a typical exam. It's consistently high-yield because renal pathology intersects with multiple organ systems.
Should I memorize all the glomerulonephritis subtypes?
Focus on the big 6: MCD, FSGS, membranous nephropathy, diabetic nephropathy (nephrotic), plus post-strep GN and IgA nephropathy (nephritic). Know their age distributions, key features, and first-line treatments.
When should I suspect RTA in a vignette?
Look for normal anion gap metabolic acidosis with specific electrolyte patterns. Type 1 RTA presents with kidney stones and inability to acidify urine, Type 4 RTA presents with hyperkalemia and diabetes or ACE inhibitor use.
What's the most high-yield nephrology topic for Step 2 CK?
AKI classification and management. It appears frequently, drives immediate clinical decisions, and integrates with other specialties (surgery, emergency medicine, critical care). Master the prerenal/intrinsic/postrenal distinction first.
How do I know when to order a renal biopsy?
Biopsy is indicated for: unexplained AKI lasting >3 weeks, nephrotic syndrome in adults (except diabetics with obvious diabetic nephropathy), rapidly progressive GN with crescents, or systemic disease with renal involvement (lupus, vasculitis).
Should I focus on adult or pediatric nephrology for Step 2 CK?
Heavily favor adult nephrology. Pediatric-specific conditions (congenital abnormalities, hereditary nephritis) appear rarely. The exception is MCD, which peaks in children but also affects adults, so know both presentations.
You can drill these nephrology patterns with targeted practice questions and lock in the clinical decision trees with high-yield nephrology flashcards. For comprehensive coverage of all Step 2 CK topics, explore our USMLE Step 2 CK study guides.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for USMLE Step 2 CK. Download free on Android and iOS.