
Nephrology (CKD, glomerular diseases) — MCQs

On this page
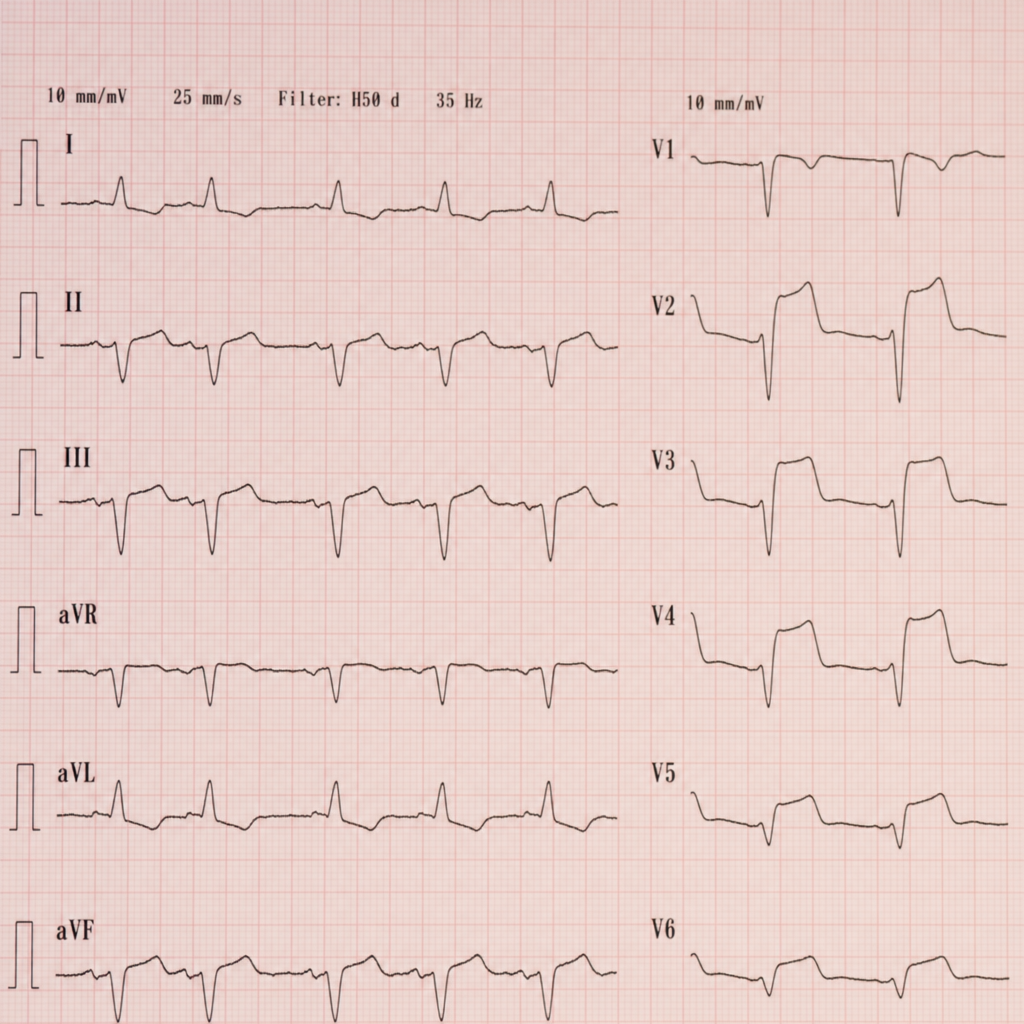
A 67-year-old man with a history of hypertension and type 2 diabetes presents to the emergency department with 2 hours of substernal chest pressure radiating to his left arm, diaphoresis, and nausea. BP is 98/60 mmHg, HR 112 bpm, RR 22/min, SpO₂ 94% on room air. A 12-lead ECG is obtained showing ST elevations in leads V1–V4 with reciprocal ST depressions in leads II, III, and aVF, consistent with an anterior STEMI. The nearest PCI-capable center is 140 minutes away by transfer, and the anticipated first-medical-contact-to-device time will exceed 120 minutes. Which of the following is the most appropriate next step in management?
Practice by Chapter
CKD classification and staging
Practice Questions
CKD etiology and pathophysiology
Practice Questions
CKD complications management
Practice Questions
Diabetic nephropathy
Practice Questions
Hypertensive nephrosclerosis
Practice Questions
Glomerulonephritis classification
Practice Questions
Primary glomerular diseases
Practice Questions
Secondary glomerular diseases
Practice Questions
Nephrotic syndrome
Practice Questions
Nephritic syndrome
Practice Questions
Acute kidney injury
Practice Questions
Renal replacement therapy
Practice Questions
Kidney transplantation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app