Back
How to Study Hematology for NEET PG 2026: Complete High-Yield Strategy for Anemia, Leukemia, Lymphoma and Bleeding Disorders
Master NEET PG hematology with this comprehensive study strategy covering anemia classification, acute leukemia differentiation, bleeding disorders, and lymphomas. Get high-yield facts, memory techniques, and a proven 30-day study schedule.
How to Study Hematology for NEET PG 2026: Complete High-Yield Strategy for Anemia, Leukemia, Lymphoma and Bleeding Disorders
You are staring at your hematology syllabus wondering how to tackle 200+ disorders, each with their own classification, pathophysiology, and clinical presentations. NEET PG dedicates 15-20 questions to hematology across internal medicine, pathology, and pediatrics — thats roughly 8% of your total score. Miss this section, and you are giving away 30-40 ranks.
The challenge isnt memorizing every blood disorder. Its identifying the 47 high-yield topics that appear repeatedly in NEET PG and building a systematic approach to differentiate between similar conditions. After analyzing 5 years of NEET PG papers, certain patterns emerge: anemia classification questions dominate (6-8 questions annually), followed by acute leukemia morphology (3-4 questions), and coagulation disorders (2-3 questions).
This guide breaks down exactly which topics to prioritize, how to approach each major category, and proven memory techniques that work specifically for hematology. You wont waste time on low-yield details, and you will nail the questions that separate toppers from the rest.
NEET PG Hematology: Topic-Wise Question Distribution
Understanding where questions come from helps you allocate study time efficiently. Here's the breakdown based on recent NEET PG papers:
Category | Annual Questions | High-Yield Subtopics | Study Priority |
|---|---|---|---|
Anemias | 6-8 | Iron deficiency, megaloblastic, hemolytic | Primary |
Acute Leukemias | 3-4 | AML vs ALL morphology, cytogenetics | Primary |
Bleeding Disorders | 2-3 | Hemophilia, vWD, platelet disorders | Secondary |
Lymphomas | 2-3 | Hodgkin vs NHL, staging | Secondary |
Chronic Leukemias | 1-2 | CML, CLL characteristics | Tertiary |
Transfusion Medicine | 1-2 | Blood grouping, cross-matching | Tertiary |
Focus 70% of your hematology time on anemias and acute leukemias. These two categories alone contribute 60% of all hematology questions.
Mastering Anemia Classification: The MCV-First Approach
Anemia questions are predictable once you master the systematic approach. NEET PG loves testing differential diagnosis between similar-presenting anemias.
Step 1: MCV Classification (90% of Questions Start Here)
Microcytic (MCV <80)
Iron deficiency anemia (most common globally)
Thalassemia (alpha and beta variants)
Anemia of chronic disease (can be normocytic too)
Sideroblastic anemia (ring sideroblasts on bone marrow)
Normocytic (MCV 80-100)
Anemia of chronic disease
Acute blood loss
Chronic kidney disease
Bone marrow infiltration
Macrocytic (MCV >100)
Megaloblastic: B12/folate deficiency
Non-megaloblastic: alcohol, hypothyroidism, liver disease
When studying anemia, use Oncourse's spaced repetition flashcards to drill the MCV cutoffs and associated findings until they are automatic.
Step 2: High-Yield Differentiating Features
Iron Studies Pattern Recognition:
Condition | Serum Iron | TIBC | Transferrin Saturation | Ferritin |
|---|---|---|---|---|
Iron deficiency | ↓ | ↑ | ↓ | ↓ |
Anemia of chronic disease | ↓ | ↓ | ↓ | ↑ |
Thalassemia | Normal/↑ | Normal | Normal/↑ | Normal/↑ |
This table alone will solve 4-5 anemia questions in NEET PG. Memorize it completely.
Step 3: Morphology Red Flags
Target cells: Thalassemia, hemoglobin C disease
Pencil cells: Iron deficiency anemia
Spherocytes: Hereditary spherocytosis, autoimmune hemolysis
Sickle cells: Sickle cell disease (obviously)
Schistocytes: Microangiopathic hemolytic anemia (TTP, HUS, DIC)
Practice identifying these on hematology MCQs where morphology images frequently appear.
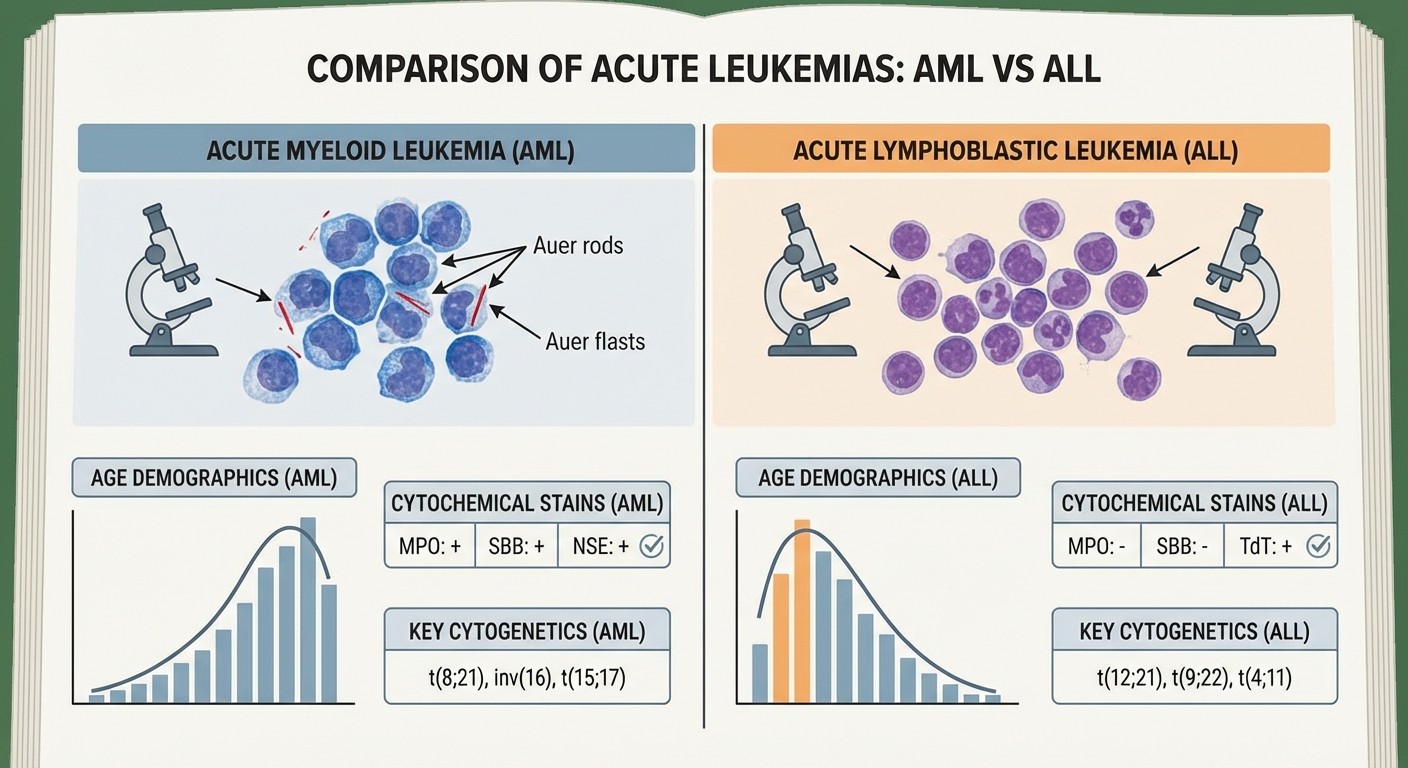
Acute Leukemia: AML vs ALL Made Simple
Acute leukemia questions focus on differentiating AML from ALL. Forget the complex WHO classification for NEET PG — focus on these high-yield differentiators.
Age and Demographics
ALL: Peak at ages 3-7 years, second peak at >50 years
AML: Median age 65 years, can occur at any age
Morphological Clues
Auer rods: Pathognomonic for AML (never seen in ALL)
Lymphoblasts in ALL: Small, uniform cells with scant cytoplasm
Myeloblasts in AML: Larger cells with more abundant cytoplasm
Cytochemical Stains
Myeloperoxidase (MPO): Positive in AML, negative in ALL
PAS stain: Block positivity in ALL, negative in AML
Sudan Black B: Positive in AML, negative in ALL
Common Cytogenetic Abnormalities
AML High-Yield:
t(15;17): APML (acute promyelocytic leukemia) — best prognosis
t(8;21): AML-M2 — good prognosis
inv(16): AML-M4Eo — good prognosis
ALL High-Yield:
t(12;21): Pre-B ALL — excellent prognosis in children
t(9;22): Philadelphia chromosome — poor prognosis
Hyperdiploidy >50 chromosomes — good prognosis
Focus your energy on these 6 cytogenetic abnormalities. They account for 80% of acute leukemia genetics questions in NEET PG.
Bleeding Disorders: Platelet vs Coagulation Patterns
NEET PG bleeding disorder questions test your ability to differentiate between platelet disorders and coagulation factor deficiencies based on clinical presentation and lab findings.
Clinical Pattern Recognition
Platelet Disorders (Thrombocytopenia/Dysfunction):
Bleeding pattern: Mucocutaneous bleeding, petechiae, purpura
Sites: Epistaxis, gum bleeding, menorrhagia, easy bruising
Onset: Immediate bleeding after trauma
Coagulation Disorders:
Bleeding pattern: Deep bleeding into muscles, joints, retroperitoneum
Sites: Hemarthrosis, intramuscular hematomas
Onset: Delayed bleeding (hours after trauma)
Laboratory Approach
Test | Platelet Disorder | Coagulation Disorder |
|---|---|---|
Platelet count | Usually <100,000 | Normal |
PT | Normal | ↑ (if factor VII, X, V, II deficiency) |
aPTT | Normal | ↑ (if factor VIII, IX, XI, XII deficiency) |
Bleeding time | ↑ | Normal |
High-Yield Bleeding Disorders
Hemophilia A (Factor VIII deficiency):
X-linked recessive inheritance
aPTT prolonged, PT normal
Deep muscle and joint bleeding
Hemophilia B (Factor IX deficiency):
X-linked recessive inheritance
Clinically identical to Hemophilia A
Distinguished only by factor assays
Von Willebrand Disease:
Most common inherited bleeding disorder
aPTT may be prolonged (if severe)
Mucocutaneous bleeding pattern
Decreased ristocetin cofactor activity
Practice bleeding disorder scenarios with Oncourse's targeted MCQs to build pattern recognition quickly.
Lymphoma: Hodgkin vs Non-Hodgkin Essentials
Lymphoma questions in NEET PG focus on classification, staging, and prognosis rather than detailed treatment protocols.
Hodgkin vs Non-Hodgkin Lymphoma
Feature | Hodgkin Lymphoma | Non-Hodgkin Lymphoma |
|---|---|---|
Age distribution | Bimodal (25-30, >55 years) | Increases with age |
Spread pattern | Contiguous spread | Random, non-contiguous |
Extranodal involvement | Uncommon | Common (40-50%) |
B symptoms | More common (30%) | Less common (20%) |
Prognosis | Better overall | Variable, generally worse |
Reed-Sternberg Cells
Pathognomonic for Hodgkin lymphoma
Large binucleated cells with prominent nucleoli
"Owl's eye" appearance on microscopy
High-Yield NHL Subtypes
1. Diffuse Large B-Cell Lymphoma (DLBCL): Most common NHL in adults 2. Follicular Lymphoma: Indolent course, t(14;18) translocation 3. Burkitt Lymphoma: Starry sky appearance, t(8;14) translocation 4. Mantle Cell Lymphoma: t(11;14) translocation, poor prognosis
30-Day Hematology Study Schedule
Week 1: Foundation (Anemias)
Days 1-3: Microcytic anemias (iron deficiency, thalassemia, ACD)
Study iron studies patterns thoroughly
Complete iron deficiency anemia lessons
Practice 50 MCQs on microcytic anemias
Days 4-5: Macrocytic anemias (megaloblastic and non-megaloblastic)
Focus on B12 vs folate deficiency differentiation
Days 6-7: Hemolytic anemias
Intravascular vs extravascular hemolysis
Hereditary spherocytosis, G6PD deficiency, sickle cell disease
Week 2: Acute Leukemias
Days 8-10: AML classification and cytogenetics Days 11-13: ALL classification and risk factors Day 14: Mixed questions comparing AML vs ALL
Use Rezzy AI tutor to clarify doubts about complex cytogenetic translocations — it explains the clinical significance of each abnormality in simple terms.
Week 3: Bleeding Disorders & Lymphomas
Days 15-17: Platelet disorders and coagulation cascade Days 18-20: Hemophilia, vWD, and acquired bleeding disorders Day 21: Hodgkin vs Non-Hodgkin lymphoma differentiation
Week 4: Integration & Revision
Days 22-25: Mixed hematology questions from previous NEET PG papers Days 26-28: Weak area reinforcement based on mock test performance Days 29-30: Final revision using spaced repetition flashcards
Memory Techniques for Hematology
Mnemonics That Actually Work
Iron Studies (FITS):
Ferritin: ↓ in iron deficiency
Iron: ↓ in iron deficiency
TIBC: ↑ in iron deficiency
Saturation: ↓ in iron deficiency
Auer Rods (AURA):
AML only (never ALL)
Unique to myeloid lineage
Rod-shaped inclusions
Acute promyelocytic leukemia (most common)
Hodgkin Lymphoma Features (HOPES):
Higher cure rate
Orderly spread (contiguous)
Peak in young adults
EEpstein-Barr virus association
SReed-Sternberg cells
Active Recall Questions
Test yourself daily with these high-yield questions:
1. What lab finding differentiates iron deficiency from anemia of chronic disease?
2. Which cytogenetic abnormality has the best prognosis in AML?
3. How do you differentiate platelet bleeding from coagulation bleeding clinically?
4. What cell is pathognomonic for Hodgkin lymphoma?
Common NEET PG Mistakes to Avoid
1. Overthinking Iron Studies
Students memorize 15 different iron study patterns when you only need to know 3: iron deficiency, anemia of chronic disease, and thalassemia. Focus on these three and move on.
2. Ignoring Clinical Context
A 65-year-old man with weight loss and anemia probably has anemia of chronic disease (due to underlying malignancy), not iron deficiency. Age and associated symptoms matter more than isolated lab values.
3. Memorizing All Cytogenetics
NEET PG tests maybe 6-7 cytogenetic abnormalities total. Focus on t(15;17) in APML, t(9;22) Philadelphia chromosome, and t(8;21) in AML. Ignore the other 50+ translocations.
4. Mixing Up Bleeding Patterns
Hemophilia = deep bleeding (joints, muscles). Thrombocytopenia = superficial bleeding (skin, mucous membranes). This distinction solves 70% of bleeding disorder questions.
High-Yield Facts for Last-Minute Revision
Anemia Quick Facts
Most common cause worldwide: Iron deficiency
Most common cause in elderly: Anemia of chronic disease
Best screening test: Complete blood count with MCV
Most sensitive test for iron deficiency: Serum ferritin <15 ng/mL
Leukemia Quick Facts
Most common leukemia in children: ALL
Most common leukemia in adults: AML
Best prognosis in AML: t(15;17) APML
Worst prognosis in ALL: t(9;22) Philadelphia positive
Lymphoma Quick Facts
Most common lymphoma overall: DLBCL (Non-Hodgkin)
Better prognosis: Hodgkin > Non-Hodgkin
Pathognomonic cell: Reed-Sternberg cells in Hodgkin
Most common site: Lymph nodes
Integrating Hematology with Other Subjects
Hematology overlaps significantly with other NEET PG subjects. Leverage these connections:
With Pediatrics
Childhood leukemias (ALL predominance)
Congenital bleeding disorders
Thalassemia and sickle cell disease
Iron deficiency in children
With Internal Medicine
Anemia workup in elderly
Complications of blood disorders
Transfusion medicine principles
Chronic leukemias in adults
With Pathology
Bone marrow morphology
Lymph node architecture
Blood film interpretation
Cytogenetic abnormalities
Study these overlaps using Oncourse's integrated lessons that connect hematology concepts across different specialties.
Frequently Asked Questions
How many questions does hematology contribute to NEET PG?
Hematology typically contributes 15-20 questions across internal medicine, pathology, and pediatrics sections. This represents about 8% of the total exam, making it a moderate-yield subject that shouldnt be ignored.
Which anemia is most commonly tested in NEET PG?
Iron deficiency anemia is the most frequently tested, appearing in 3-4 questions annually. Focus on iron studies interpretation, morphology (pencil cells), and differentiation from anemia of chronic disease.
Is cytogenetics important for NEET PG hematology?
Yes, but only specific high-yield translocations. Focus on t(15;17) for APML, t(9;22) Philadelphia chromosome, t(8;21) for AML, and t(14;18) for follicular lymphoma. These 4 translocations cover 90% of genetics questions.
How do I differentiate between AML and ALL quickly?
Look for Auer rods (present only in AML), check myeloperoxidase stain (positive in AML, negative in ALL), and consider age (ALL peaks in children, AML in elderly). These three features solve most differentiation questions.
Should I memorize all bleeding time values?
No. Focus on the pattern: bleeding time is prolonged in platelet disorders (thrombocytopenia, vWD) and normal in coagulation disorders (hemophilia). The actual values are less important than understanding the concept.
How important are lymphoma staging systems for NEET PG?
Ann Arbor staging basics are sufficient. Know that stage I-II is limited disease (better prognosis) and stage III-IV is advanced disease (worse prognosis). Detailed staging criteria are rarely tested.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for NEET PG. Download free on Android and iOS.