How to Study Surgery for NEET PG 2026: Complete High-Yield Strategy
Master surgery for NEET PG 2026 with this complete strategy guide covering high-yield topics, Bailey & Love chapter priorities, trauma patterns, and image-based question techniques for maximum marks.
How to Study Surgery for NEET PG 2026: Complete High-Yield Strategy
You are probably staring at your copy of Bailey & Love, wondering how you will ever memorise 1,500 pages of surgical procedures. Here's what most students dont realise: surgery accounts for 15-20 questions in NEET PG 2026 — making it the highest-scoring clinical subject. Yet 80% of students waste time on low-yield procedures that never appear in exams.
NEET PG surgery isnt about memorising every surgical technique. It's about pattern recognition. The examiners test specific clinical scenarios, intraoperative findings, and post-operative complications through image-based MCQs and clinical vignettes. Master the right 30% of surgery content, and you will score 85%+ in this section.
This guide gives you the precise topic priority map that toppers use — what to master, what to skim, and what to skip entirely.
Why Surgery is Your NEET PG Scoring Goldmine
Surgery delivers 15-20 marks in NEET PG 2026, distributed across these systems:
Gastrointestinal Surgery: 4-5 questions (appendicitis, hernia, gallbladder, colorectal)
Trauma & Emergency Surgery: 3-4 questions (ATLS protocols, head injury, abdominal trauma)
Orthopedics: 2-3 questions (fracture classification, spine injuries)
Urology: 2-3 questions (stone disease, BPH, tumors)
Breast & Endocrine Surgery: 2-3 questions (thyroid, breast cancer staging)
Vascular Surgery: 1-2 questions (DVT, peripheral vascular disease)
Pediatric Surgery: 1-2 questions (congenital anomalies)
Unlike medicine where you need broad knowledge across 20 subspecialties, surgery questions cluster around specific high-yield scenarios. Master these patterns, and surgery becomes your highest return-on-investment subject.
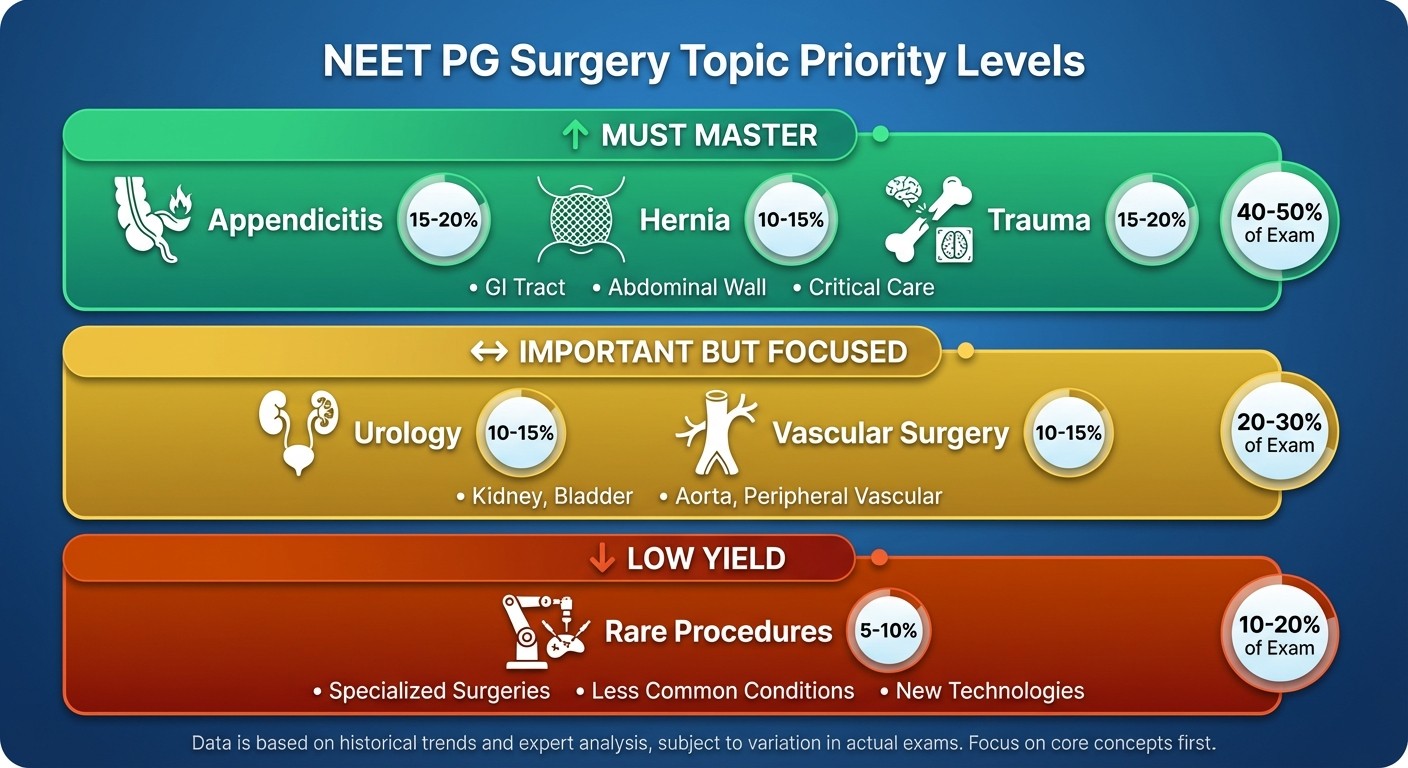
High-Yield vs Low-Yield Surgery Topics
The NEET PG surgery blueprint hasnt changed in 5 years. Here's your priority map:
Must-Master Topics (80% of questions come from here):
Gastrointestinal Surgery:
Acute appendicitis (clinical presentation, Alvarado score, complications)
Inguinal hernia (types, repair techniques, complications)
Gallstone disease (cholelithiasis, cholecystitis, choledocholithiasis)
Peptic ulcer disease (indications for surgery, complications)
Colorectal cancer (staging, lymph node clearance, adjuvant therapy)
Inflammatory bowel disease (surgical indications, complications)
Trauma & Emergency Surgery:
Head injury (Glasgow Coma Scale, intracranial pressure management)
Abdominal trauma (FAST scan interpretation, organ-specific injuries)
Thoracic trauma (pneumothorax, hemothorax, cardiac tamponade)
ATLS protocols (primary survey, resuscitation priorities)
Breast Surgery:
Breast cancer (TNM staging, sentinel lymph node biopsy, treatment algorithms)
Benign breast disease (fibroadenoma, phyllodes tumor)
Endocrine Surgery:
Thyroid disorders (thyroidectomy indications, complications)
Parathyroid surgery (hyperparathyroidism, surgical anatomy)
Important but Focused Topics (15% of questions):
Urology: Stone disease, BPH, renal tumors
Vascular Surgery: DVT prophylaxis, peripheral arterial disease
Pediatric Surgery: Pyloric stenosis, intussusception, anorectal malformations
Low-Yield Topics (Skip or Skim):
Detailed surgical techniques and step-by-step procedures
Rare surgical conditions (<1% prevalence)
Historical surgical approaches
Complex reconstructive procedures
Must-Do Chapters: Bailey & Love vs SRB Manual
Most students get paralysed choosing between textbooks. Here's the chapter-wise breakdown that works:
Bailey & Love's Surgery (27th Edition) - Core Chapters:
Part 1: Principles (Chapters 1-14)
Chapter 1: History and clinical examination ✓
Chapter 4: Shock and resuscitation ✓
Chapter 8: Principles of operative surgery ✓
Chapter 11: Surgical site infection ✓
Part 2: Investigation and Diagnosis (Chapters 15-20)
Chapter 15: Imaging in surgery ✓ (focus on CT/MRI interpretation)
Chapter 17: Tissue sampling and staging ✓
Part 3: Trauma (Chapters 21-32)
Chapter 22: Early assessment and management of trauma ✓ (ATLS focus)
Chapter 24: Head and spine injury ✓
Chapter 26: Torso trauma ✓
Part 8: Breast and Endocrine (Chapters 77-84)
Chapter 80: Breast cancer ✓ (staging, treatment algorithms)
Chapter 81: The thyroid gland ✓
SRB's Manual of Surgery (6th Edition) - Quick Review:
Use SRB for rapid revision, not primary reading. Focus on:
Chapter 3: Shock and fluid therapy (page 51-78)
Chapter 35: Acute appendicitis (page 789-812)
Chapter 42: Inguinal hernia (page 943-968)
Chapter 58: Breast diseases (page 1247-1289)
Pro tip: Bailey & Love for understanding concepts, SRB for exam patterns and quick facts. Oncourse's surgery lessons break down these exact chapters into digestible modules that you can review between clinical postings.
Surgical Anatomy Quick-Wins
NEET PG loves testing anatomical landmarks through clinical scenarios. Master these high-yield anatomy points:
Surface Anatomy & Landmarks:
McBurney's point: 1/3rd distance from ASIS to umbilicus (appendicitis)
Calot's triangle: Boundaries and contents (cholecystectomy anatomy)
Triangle of pain: Lateral to gonadal vessels in laparoscopic hernia repair
Hesselbach's triangle: Medial boundary of inguinal canal
Surgical Incisions (Image-Based Questions):
Kocher's incision: Right subcostal (cholecystectomy)
Pfannenstiel incision: Suprapubic transverse (gynecologic surgery)
Midline laparotomy: Most versatile abdominal approach
Fascial Layers & Closure:
Abdominal wall layers: Skin → Camper's → Scarpa's → External oblique → Internal oblique → Transversalis → Peritoneum
Mass closure technique: All fascial layers except skin in single continuous suture
When reviewing surgical anatomy, use Oncourse's surgery flashcards for spaced repetition — anatomical landmarks stick better when tested repeatedly rather than cramming from diagrams.
Trauma and Emergency Surgery MCQ Patterns
Emergency surgery questions follow ATLS protocols religiously. Here's how NEET PG tests this:
Clinical Vignette Structure:
1. Mechanism of injury: RTA, fall from height, penetrating trauma 2. Initial presentation: Vital signs, conscious level, obvious injuries 3. Primary survey findings: Airway, breathing, circulation abnormalities 4. Investigation results: CT findings, X-ray abnormalities 5. Question: Next step in management or most likely diagnosis
Must-Know ATLS Concepts:
Primary Survey (ABCDE):
Airway: Cervical spine immobilisation, jaw thrust vs head tilt
Breathing: Tension pneumothorax vs simple pneumothorax management
Circulation: Shock classification, fluid resuscitation protocols
Disability: Glasgow Coma Scale scoring, pupil assessment
Exposure: Log roll technique, hypothermia prevention
Shock Classifications:
Class I: <15% blood loss, normal vital signs
Class II: 15-30% loss, tachycardia, narrow pulse pressure
Class III: 30-40% loss, hypotension, oliguria
Class IV: >40% loss, profound shock, altered mental status
High-Yield Trauma Scenarios:
Head Injury Patterns:
Extradural hematoma: Lucid interval → deterioration
Subdural hematoma: Progressive decline in elderly
Subarachnoid hemorrhage: Thunderclap headache, neck stiffness
Abdominal Trauma Red Flags:
Seat belt sign: Chance fracture + bowel injury
Grey Turner's sign: Retroperitoneal bleeding
Cullen's sign: Intraperitoneal bleeding
Practice trauma scenarios using Oncourse's adaptive MCQ platform — the AI explains ATLS decision trees step-by-step, so you understand why each management option is correct or wrong.
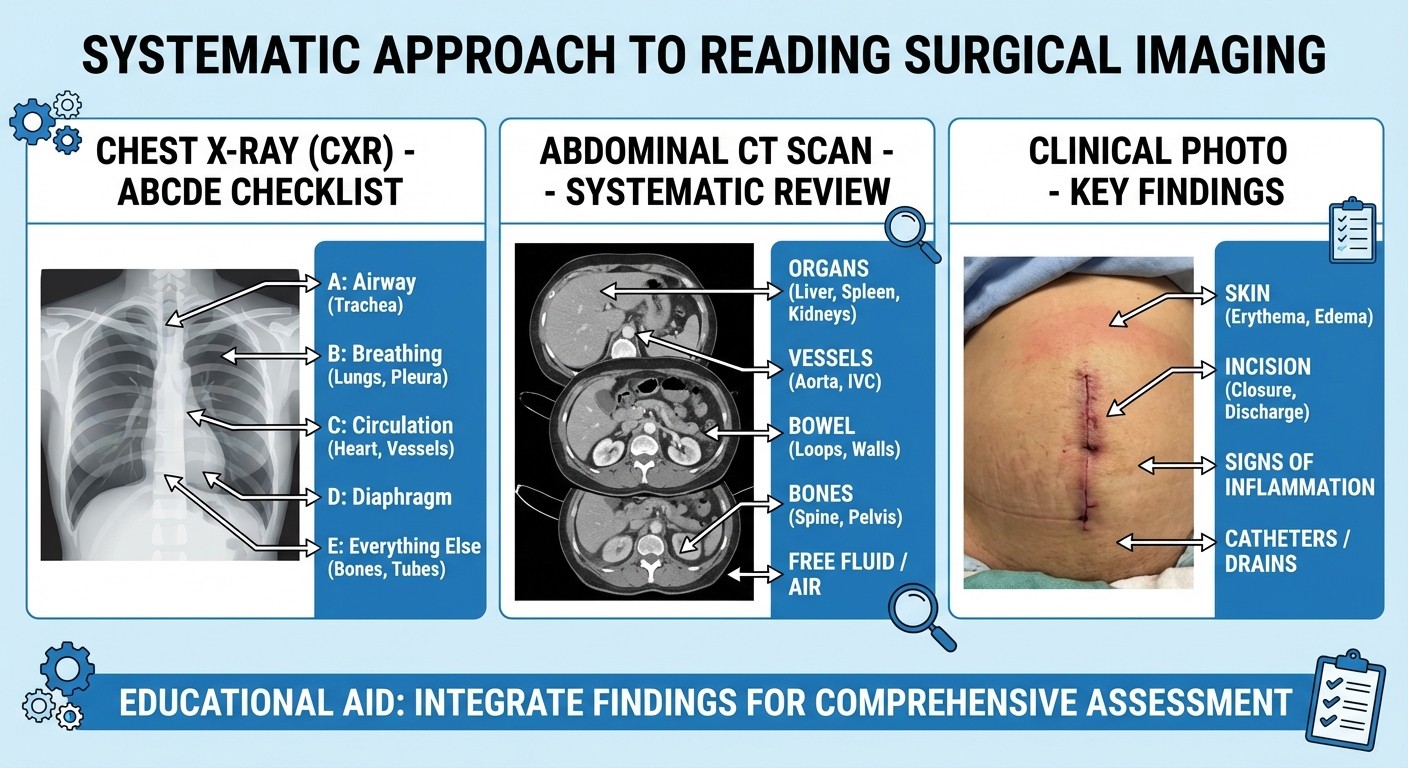
Image-Based Surgical Question Strategy
40% of surgery questions include radiological images or clinical photographs. Here's how to decode them systematically:
X-Ray Interpretation Framework:
Chest X-Rays: 1. Technique: PA vs AP, inspiratory effort, rotation 2. Systematic review: Airway → Breathing → Circulation → Diaphragm → Everything else 3. Trauma findings: Pneumothorax (absent lung markings), hemothorax (fluid level), widened mediastinum (aortic injury) Abdominal X-Rays: 1. Gas patterns: Small bowel vs large bowel dilatation 2. Obstruction signs: Air-fluid levels, distended loops 3. Foreign bodies: Radio-opaque vs radio-lucent objects
CT Scan High-Yield Findings:
Head CT:
Extradural: Lemon-shaped hyperdensity
Subdural: Crescent-shaped hyperdensity
Intracerebral: Irregular hyperdensity with surrounding edema
Abdominal CT:
Appendicitis: Appendicular wall thickening, fat stranding
Gallbladder pathology: Wall thickening, pericholecystic fluid
Bowel obstruction: Transition point, proximal dilatation
Clinical Photography Patterns:
Skin Lesions: Melanoma ABCDE criteria, basal cell vs squamous cell carcinoma Hernias: Inguinal vs femoral location, irreducible vs strangulated appearance Breast Lumps: Skin changes (peau d'orange), nipple retraction, lymphadenopathy Study tip: Create a mental checklist for each image type. When practicing MCQs, force yourself to describe what you see before looking at the options — this prevents getting distracted by obviously wrong answers.
Oncology Surgery High-Yield Topics
Surgical oncology appears in 3-4 questions per NEET PG exam. Focus on these scoring concepts:
TNM Staging Essentials:
Breast Cancer:
T1: ≤2cm, T2: 2-5cm, T3: >5cm, T4: chest wall/skin involvement
N1: 1-3 axillary nodes, N2: 4-9 nodes, N3: ≥10 nodes
M1: Distant metastases (bone, liver, lung, brain)
Colorectal Cancer:
T1: Submucosa, T2: Muscularis propria, T3: Subserosa, T4: Adjacent organs
N categories based on number of positive lymph nodes
Dukes staging: A (mucosa/submucosa), B (muscle), C (lymph nodes), D (distant)
Lymph Node Management:
Sentinel Lymph Node Biopsy:
Indications: Early breast cancer (T1-T2, clinically node-negative)
Technique: Blue dye + radioisotope injection
Positive result: Requires axillary lymph node dissection
Lymph Node Clearance Levels:
Level I: Lateral to pectoralis minor
Level II: Behind pectoralis minor
Level III: Medial to pectoralis minor
Adjuvant Therapy Decisions:
Breast Cancer:
Hormone receptor positive: Tamoxifen/Aromatase inhibitors
HER2 positive: Trastuzumab-based therapy
Triple negative: Chemotherapy only
Colorectal Cancer:
Stage II high-risk: Consider adjuvant chemotherapy
Stage III: Definite adjuvant chemotherapy
Rectal cancer: Neoadjuvant chemoradiotherapy
Remember the staging algorithms through active recall — Oncourse's spaced repetition system presents cancer staging scenarios at optimal intervals, so you dont forget TNM criteria during exam stress.
Last 45-Day Surgery Sprint Plan
With 45 days remaining, here's your high-impact revision strategy:
Week 1-2: Foundation Building
Days 1-7: Complete Bailey & Love trauma chapters (22, 24, 26)
Days 8-14: Master GI surgery basics (appendicitis, hernia, gallbladder)
Daily target: 2 hours theory + 50 MCQs from mixed surgery topics
Week 3-4: Pattern Recognition
Days 15-21: Image-based questions marathon (100 images/day)
Days 22-28: Clinical vignette practice (focus on management decisions)
Daily target: 1 hour theory review + 75 MCQs + image interpretation
Week 5-6: High-Yield Consolidation
Days 29-35: Oncology surgery + staging systems
Days 36-42: Emergency surgery protocols (ATLS framework)
Daily target: 30 minutes theory + 100 MCQs + weak area targeting
Week 7: Exam Simulation
Days 43-45: Full-length mock tests with surgery sections
Review pattern: Analyse every wrong answer, create weakness list
Final prep: Memorise high-yield facts (anatomy landmarks, staging criteria)
Daily Routine Structure:
Morning (6-8 AM): Fresh topic reading (Bailey & Love chapters)
Afternoon (2-4 PM): MCQ practice with immediate review
Evening (8-9 PM): Image interpretation + flashcard review
Use Oncourse's adaptive question bank to target your weak areas — the AI identifies which surgical subtopics need more practice and serves questions accordingly, so you spend time on gaps rather than topics you have already mastered.
Advanced MCQ Pattern Recognition
NEET PG surgery questions follow predictable templates. Master these patterns:
Clinical Vignette Structure Analysis:
Type 1: Diagnostic Questions
Patient demographics + chief complaint
Physical examination findings
Investigation results
Question: "Most likely diagnosis?"
Type 2: Management Questions
Established diagnosis + current status
Complicating factors or contraindications
Available treatment options
Question: "Next best step in management?"
Type 3: Complications/Prognosis
Post-operative scenario
Unexpected findings or patient deterioration
Timeline and associated symptoms
Question: "Most likely complication?" or "Poor prognostic factor?"
Red Flag Keywords That Signal Answers:
Diagnostic Clues:
"Sudden onset" → Think vascular emergency (ruptured AAA, mesenteric ischemia)
"Gradual onset" → Think malignancy or chronic inflammation
"Young female" + abdominal pain → Think appendicitis, ovarian pathology
"Elderly male" + urinary symptoms → Think BPH, prostate cancer
Management Triggers:
"Hemodynamically unstable" → Immediate surgery/resuscitation
"Stable patient" → Conservative management or elective surgery
"Failed conservative management" → Escalate to surgical intervention
The key insight: NEET PG doesnt test obscure knowledge — it tests your ability to apply standard protocols to clinical scenarios. When Oncourse's Rezzy AI tutor explains why an answer is wrong, pay attention to the decision tree logic, not just the facts.
Frequently Asked Questions
How many surgery questions appear in NEET PG 2026?
Surgery typically accounts for 15-20 questions out of 200 total questions in NEET PG, making it one of the highest-weighted clinical subjects after medicine and pediatrics.
Should I prioritise Bailey & Love or SRB Manual for surgery preparation?
Use Bailey & Love for conceptual understanding and primary reading, then SRB Manual for quick revision and exam-pattern familiarisation. Bailey & Love provides depth, while SRB gives you the exam-focused perspective.
How important is surgical anatomy for NEET PG?
Surgical anatomy accounts for 20-30% of surgery questions through clinical correlation. Focus on surface landmarks, fascial planes, and anatomical relations that have direct clinical significance rather than detailed developmental anatomy.
What percentage of surgery questions are image-based?
Approximately 40% of surgery questions include radiological images (X-rays, CT scans) or clinical photographs. Systematic image interpretation skills are essential for scoring well in surgery.
How should I balance trauma surgery with elective surgery topics?
Trauma and emergency surgery contribute 3-4 questions per exam and follow ATLS protocols strictly. Spend 30% of your surgery study time on trauma, 70% on elective surgery topics like GI, breast, and endocrine surgery.
Is it worth studying rare surgical procedures for NEET PG?
No. Focus on common surgical conditions that have high clinical prevalence. Rare procedures (<1% prevalence) rarely appear in NEET PG and studying them wastes precious preparation time.
---
Surgery success in NEET PG 2026 comes from targeted preparation, not exhaustive reading. Master the high-yield topics, practice pattern recognition through MCQs, and develop systematic approaches to clinical vignettes and image interpretation.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for NEET PG. Download free on Android and iOS.