How to Study Nephrology for NEET PG 2026: Glomerulonephritis, Renal Failure, Electrolytes and High-Yield MCQ Strategy
Master nephrology for NEET PG 2026 with this comprehensive guide covering glomerulonephritis classification, AKI vs CKD, electrolyte disorders, and proven MCQ strategies for high-yield topics.
How to Study Nephrology for NEET PG 2026: Glomerulonephritis, Renal Failure, Electrolytes and High-Yield MCQ Strategy
You are probably staring at nephrology thinking it feels like learning a foreign language. The kidney handles 180 litres of filtrate daily, maintains precise electrolyte balance, and when it goes wrong, the presentations span everything from subtle lab changes to life-threatening emergencies. NEET PG 2026 loves testing nephrology because it bridges basic science with clinical medicine perfectly.
Here's what makes nephrology different from other subjects: the pathophysiology matters more than memorizing isolated facts. You cant just learn that "proteinuria = nephrotic syndrome" and expect to score. You need to understand why minimal change disease responds to steroids while focal segmental glomerulosclerosis doesnt, and how that translates into MCQ stems.
NEET PG typically includes 8-12 nephrology questions across Internal Medicine, Pediatrics, and Biochemistry. The highest-yield topics are glomerulonephritis classification, acute kidney injury causes, electrolyte disorders, and diuretics mechanisms. Master these four areas and you will handle 70% of nephrology questions confidently.
This guide breaks down nephrology into digestible, high-yield sections with specific MCQ strategies for each topic. We will cover the pathophysiology that actually gets tested, not textbook details that waste your time.
Understanding NEET PG Nephrology Question Patterns
NEET PG nephrology questions follow predictable patterns. Most questions test your ability to differentiate between similar conditions using clinical vignettes and lab values.
Common question types:
Glomerulonephritis classification based on urinalysis and biopsy findings
AKI vs CKD differentiation using creatinine trends and imaging
Electrolyte disorder interpretation with ECG changes
Diuretic mechanisms and side effect profiles
Renal tubular acidosis types based on urine pH and anion gap
The key insight: NEET PG rarely asks direct definitions. Instead, they present clinical scenarios where you need to apply nephrology concepts to reach the diagnosis. For example, instead of asking "What is nephrotic syndrome?", they will give you a 5-year-old with facial puffiness, proteinuria 4+, and hypoalbuminemia, then ask about the most likely diagnosis.
Understanding this pattern changes how you study. Focus on connecting pathophysiology to clinical presentations rather than memorizing isolated facts. When you encounter electrolyte questions, the adaptive question bank surfaces the most-tested scenarios and adjusts to your weak areas, letting you master these connections in 3-4 targeted revision sessions.
High-Yield Glomerulonephritis Classification
Glomerulonephritis questions are NEET PG favorites because they test pattern recognition across multiple systems. The key is understanding the nephritic vs nephrotic spectrum, not memorizing every rare variant.
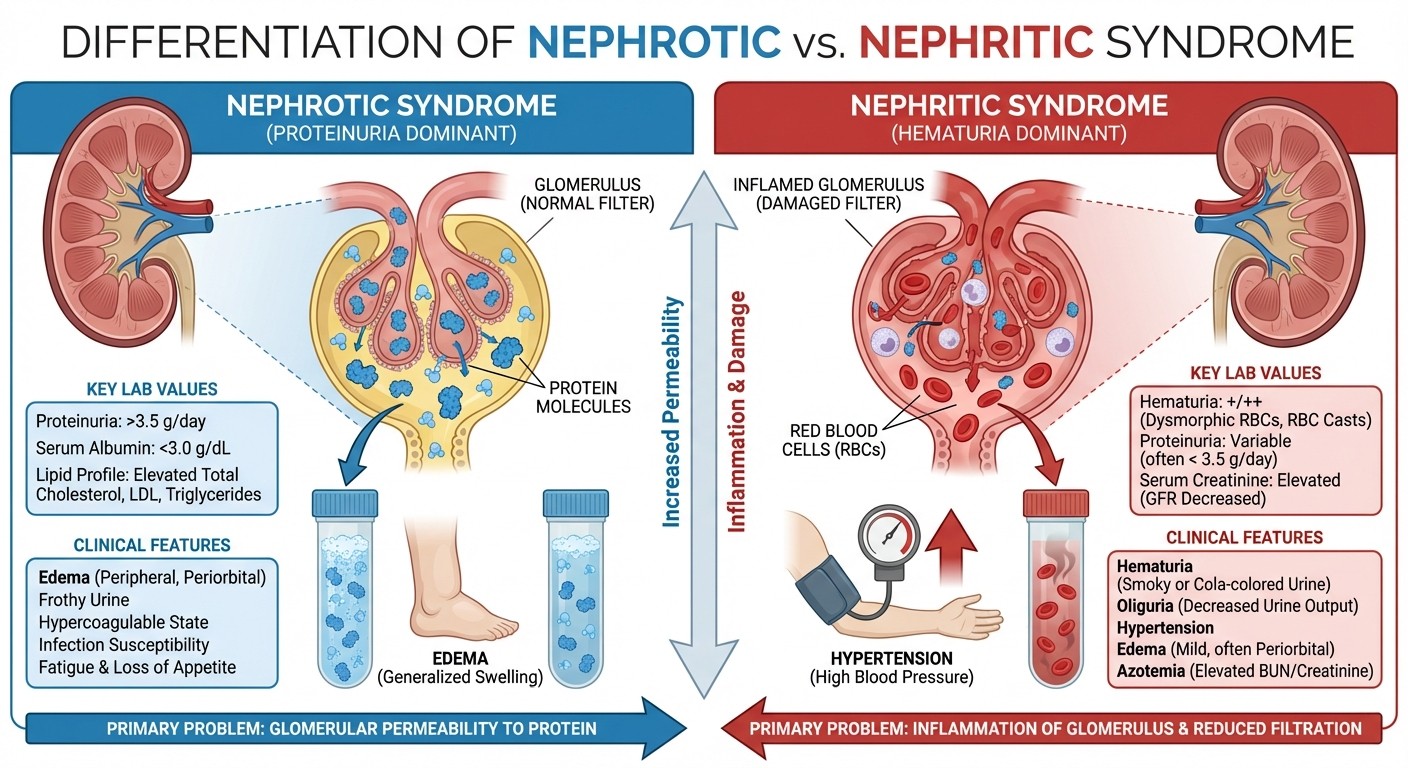
Nephrotic vs Nephritic Syndrome Differentiation
Nephrotic syndrome (proteinuria dominant):
Proteinuria >3.5g/day (massive)
Hypoalbuminemia <3g/dL
Edema (facial, pedal)
Hyperlipidemia
Minimal hematuria
Nephritic syndrome (hematuria dominant):
Proteinuria <3g/day (mild to moderate)
Gross or microscopic hematuria
RBC casts in urine
Hypertension
Oliguria with fluid retention
Most-Tested Glomerulonephritis Types
Minimal Change Disease (MCD):
Most common nephrotic syndrome in children
Normal light microscopy
Responds to steroids (steroid-sensitive)
Key MCQ clue: child with sudden onset facial swelling
Focal Segmental Glomerulosclerosis (FSGS):
Most common cause of steroid-resistant nephrotic syndrome
Associated with HIV, heroin use, obesity
Poor prognosis, progresses to ESRD
MCQ clue: African American with nephrotic syndrome + drug history
Membranous Nephropathy:
Most common nephrotic syndrome in adults
Associated with hepatitis B, malignancy, drugs (NSAIDs, gold)
"Spike and dome" appearance on electron microscopy
MCQ clue: elderly male with cancer history
Post-infectious Glomerulonephritis:
Most common acute nephritic syndrome in children
Follows streptococcal infection by 1-2 weeks
Low C3, elevated ASO titers
MCQ clue: child with recent sore throat + cola-colored urine
For glomerulonephritis practice, work through nephrology MCQs and detailed pathophysiology lessons to connect biopsy findings with clinical presentations.
Acute Kidney Injury (AKI) and Chronic Kidney Disease (CKD)
AKI questions test your ability to identify causes and classify severity, while CKD questions focus on staging and complications. NEET PG loves testing the distinction between these two conditions.
AKI Classification and Causes
KDIGO AKI Definition:
Serum creatinine increase ≥0.3 mg/dL within 48 hours, OR
Serum creatinine increase ≥1.5x baseline within 7 days, OR
Urine output <0.5 mL/kg/hr for 6 hours
AKI Causes (Pre-renal, Intrinsic, Post-renal): Pre-renal (60-70% of AKI):
Volume depletion (dehydration, bleeding)
Heart failure, cirrhosis
NSAIDs, ACE inhibitors
FeNa <1%, BUN:Creatinine >20:1
Intrinsic Renal (25-30%):
Acute tubular necrosis (ATN) - most common
Acute interstitial nephritis (drug-induced)
Glomerulonephritis
FeNa >2%, muddy brown casts in ATN
Post-renal (5-10%):
Obstruction (stones, BPH, malignancy)
Bilateral involvement needed for AKI
Hydronephrosis on ultrasound
The concept maps and explanations link each AKI cause to its pathophysiology and help you understand why FeNa differentiates pre-renal from intrinsic causes - it is not just a random lab value to memorize.
CKD Staging and Complications
CKD Staging (based on eGFR):
Stage 1: eGFR ≥90 (kidney damage with normal GFR)
Stage 2: eGFR 60-89 (mild decrease)
Stage 3a: eGFR 45-59 (moderate decrease)
Stage 3b: eGFR 30-44 (moderate decrease)
Stage 4: eGFR 15-29 (severe decrease)
Stage 5: eGFR <15 (kidney failure)
High-Yield CKD Complications by Stage:
Stage 3: Anemia, bone disease starts
Stage 4: Acidosis, hyperkalemia, prepare for RRT
Stage 5: Uremia, indication for dialysis/transplant
MCQ Pearl: NEET PG often tests when to start specific treatments:
ACE inhibitors: any stage with proteinuria
EPO for anemia: Hb <10 g/dL (usually stage 3-4)
Phosphate binders: Stage 4-5
Dialysis: eGFR <10 or uremic symptoms
Study acute renal failure management and renal replacement therapy for detailed protocols and indications.
Electrolyte Disorders: Sodium, Potassium, and Acid-Base
Electrolyte questions are high-yield because they appear across multiple subjects and test physiological understanding. Focus on the clinical presentations and ECG changes rather than complex calculations.
Sodium Disorders
Hyponatremia (Na+ <135 mEq/L):
Hypovolemic: Diuretics, diarrhea, burns
Euvolemic: SIADH, hypothyroidism, drugs
Hypervolemic: Heart failure, cirrhosis, nephrotic syndrome
SIADH Criteria (most tested):
Hyponatremia with concentrated urine (>300 mOsm/kg)
Normal kidney, thyroid, adrenal function
No diuretic use
Urine Na+ >20 mEq/L
Hypernatremia (Na+ >145 mEq/L):
Usually due to free water loss
Diabetes insipidus (central vs nephrogenic)
Osmotic diuresis
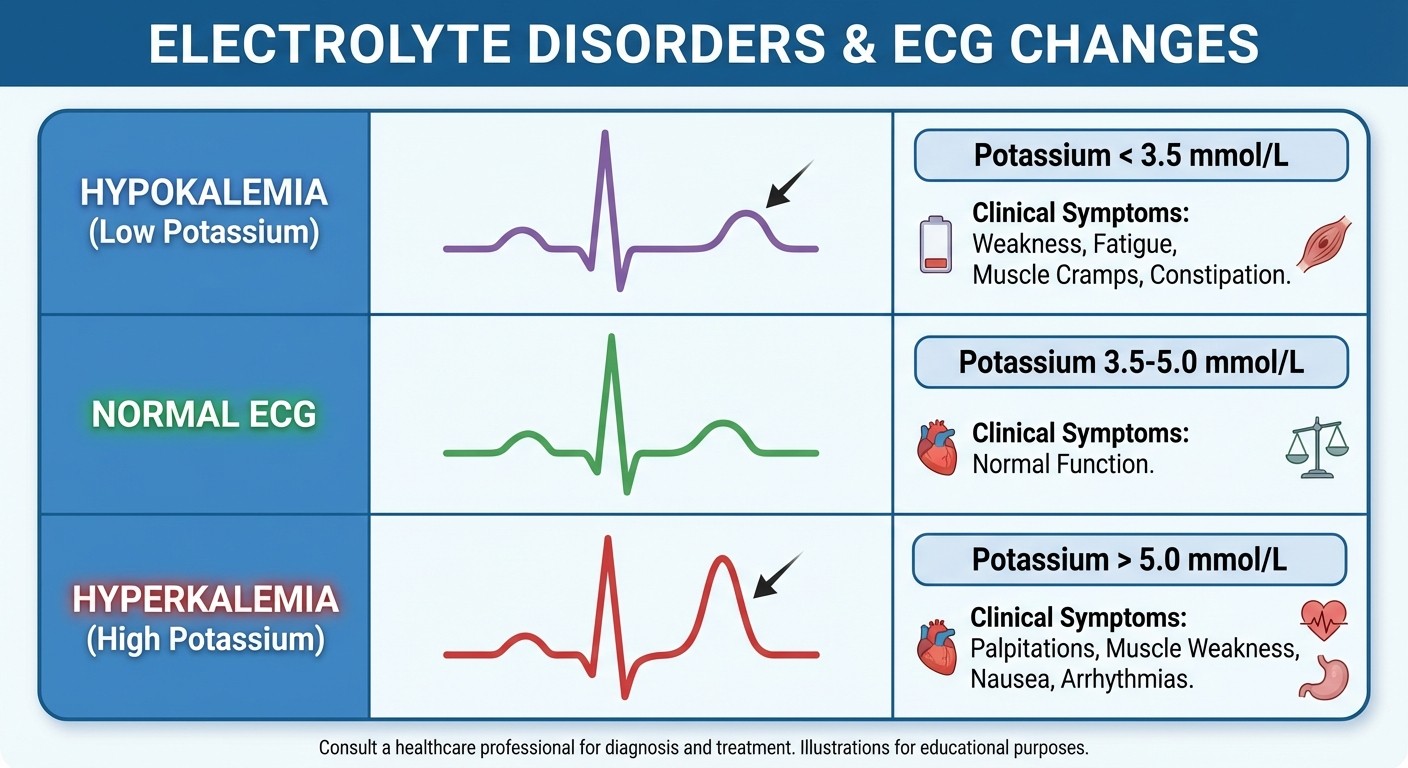
Potassium Disorders and ECG Changes
Hypokalemia (K+ <3.5 mEq/L):
Causes: Diuretics, diarrhea, hyperaldosteronism
ECG: U waves, flat T waves, ST depression
Symptoms: Weakness, cramping, polyuria
Hyperkalemia (K+ >5.5 mEq/L):
Causes: Renal failure, ACE inhibitors, K+-sparing diuretics
ECG: Peaked T waves → wide QRS → sine wave
Emergency treatment: Calcium gluconate + insulin/glucose
MCQ Strategy: NEET PG loves giving ECG strips with electrolyte disorders. Memorize the specific ECG changes for each electrolyte abnormality - they are highly testable and easy points once you know the patterns.
Practice electrolyte interpretation with sodium and water balance lessons and potassium balance scenarios.
Renal Tubular Acidosis (RTA)
RTA questions test your understanding of acid-base physiology. Focus on the key differentiating features rather than complex pathways.
Type 1 RTA (Distal):
Cannot acidify urine (urine pH >5.5)
Normal anion gap metabolic acidosis
Hypokalemia, hypocitraturia
Complications: Nephrolithiasis, nephrocalcinosis
Type 2 RTA (Proximal):
Bicarbonate wasting
Can acidify urine when bicarbonate depleted
Associated with Fanconi syndrome
Complications: Growth retardation, rickets
Type 4 RTA (Hyperkalemic):
Aldosterone deficiency/resistance
Hyperkalemia (differentiating feature)
Mild metabolic acidosis
Associated with diabetes, drugs (ACE inhibitors, NSAIDs)
Performance analytics track your accuracy across different RTA types so you know whether to focus more time on the pathophysiology connections or just drilling the clinical patterns.
Diuretics: Mechanisms and Clinical Applications
Diuretic questions are favorites because they test pharmacology, physiology, and clinical medicine together. Focus on the site of action and specific side effects for each class.
Diuretic Classifications and Mechanisms
Loop Diuretics (Furosemide, Bumetanide):
Site: Thick ascending limb (Na-K-2Cl cotransporter)
Most potent diuretics
Side effects: Hypokalemia, hyponatremia, ototoxicity, hyperuricemia
Clinical use: Heart failure, pulmonary edema
Thiazide Diuretics (HCTZ, Chlorthalidone):
Site: Distal convoluted tubule (Na-Cl cotransporter)
Side effects: Hypokalemia, hyperuricemia, hyperglycemia, hyperlipidemia
Clinical use: Hypertension (first-line), heart failure
Potassium-Sparing Diuretics:
Spironolactone: Aldosterone receptor antagonist
Amiloride: ENaC blocker
Side effects: Hyperkalemia, gynecomastia (spironolactone)
Clinical use: Combination with loop/thiazide diuretics
Carbonic Anhydrase Inhibitors (Acetazolamide):
Site: Proximal tubule
Weak diuretic effect
Clinical use: Glaucoma, altitude sickness, epilepsy
High-Yield Diuretic Pearls
MCQ Strategy for Diuretics:
1. Identify the clinical scenario (heart failure vs hypertension vs edema)
2. Match the diuretic class to the appropriate clinical use
3. Look for specific side effects in the answer choices
4. Remember drug interactions (lithium + thiazides = lithium toxicity)
Common NEET PG Diuretic Scenarios:
Heart failure patient with loop diuretic + spironolactone combination
Hypertensive patient starting thiazide with electrolyte monitoring
Diuretic resistance in heart failure (increase dose vs add second agent)
Side effect identification (gynecomastia = spironolactone)
Master diuretic pharmacology through fluid and electrolyte disorder lessons and targeted MCQ practice.
MCQ Strategy for Nephrology Topics
Nephrology MCQs require a systematic approach because they often present complex clinical scenarios with multiple lab values and imaging findings.
Step-by-Step MCQ Approach
Step 1: Identify the Chief Complaint
Oliguria/anuria → Think AKI vs CKD
Edema + proteinuria → Glomerular disease
Electrolyte abnormality → Specific disorder workup
Step 2: Analyze Key Lab Values
Creatinine trend (acute rise vs chronic elevation)
Urine analysis (RBCs, protein, casts)
Electrolytes (Na, K, Cl, HCO3)
Fractional excretion of sodium (FeNa)
Step 3: Look for Diagnostic Clues
Age group (children = post-infectious GN, MCD)
Associated conditions (diabetes, hypertension, drugs)
Imaging findings (hydronephrosis, kidney size)
Response to treatment (steroids in MCD)
Common NEET PG Nephrology MCQ Traps
Trap 1: AKI vs CKD Confusion
Solution: Look for creatinine timeline and kidney size
AKI: Recent rise, normal-sized kidneys
CKD: Gradual rise, small kidneys
Trap 2: Electrolyte Disorder Causes
Solution: Always consider medications in the history
ACE inhibitors → Hyperkalemia
Diuretics → Hypokalemia/hyponatremia
Trap 3: Glomerulonephritis Classification
Solution: Focus on age, presentation pattern, and lab findings
Don't get lost in rare biopsy findings
Trap 4: RTA Type Confusion
Solution: Use hyperkalemia as the key differentiator
Only Type 4 RTA has hyperkalemia
The adaptive question bank identifies these common mistake patterns and gives you targeted practice on your weak areas, so you dont keep falling for the same traps across different question formats.
Creating Your Nephrology Study Schedule
A systematic approach to nephrology ensures you cover high-yield topics without getting lost in low-yield details.
Week-by-Week Nephrology Plan
Week 1: Foundation Building
Day 1-2: Glomerulonephritis classification (nephrotic vs nephritic)
Day 3-4: AKI causes and classification
Day 5-6: CKD staging and complications
Day 7: Practice MCQs on basic concepts
Week 2: Electrolyte Mastery
Day 1-2: Sodium disorders (SIADH, diabetes insipidus)
Day 3-4: Potassium disorders and ECG changes
Day 5-6: Renal tubular acidosis types
Day 7: Mixed electrolyte disorder practice
Week 3: Advanced Topics
Day 1-2: Diuretic mechanisms and side effects
Day 3-4: Renal replacement therapy indications
Day 5-6: Integrated case scenarios
Day 7: Full-length nephrology practice test
Daily Study Structure
Morning (45 minutes):
Read one nephrology topic from your textbook
Make connection diagrams linking pathophysiology to clinical presentation
Review relevant lessons for detailed explanations
Afternoon (30 minutes):
Solve 20-25 MCQs on the morning's topic
Review explanations for both correct and incorrect options
Note down high-yield facts and clinical pearls
Evening (15 minutes):
Quick revision using flashcards
Focus on weak areas identified through performance tracking
This schedule ensures you cover all major nephrology topics while building pattern recognition through consistent MCQ practice.
Frequently Asked Questions
How many nephrology questions appear in NEET PG 2026?
NEET PG typically includes 8-12 nephrology questions distributed across Internal Medicine (5-7 questions), Pediatrics (2-3 questions), and Biochemistry (1-2 acid-base questions). The subject carries moderate weightage but high-yield topics like glomerulonephritis and electrolyte disorders are consistently tested.
Which nephrology topics have the highest yield for NEET PG?
Focus on glomerulonephritis classification (nephrotic vs nephritic syndrome), acute kidney injury causes and classification, electrolyte disorders with ECG changes, diuretic mechanisms and side effects, and renal tubular acidosis types. These five topics cover approximately 70% of nephrology questions in NEET PG.
How should I differentiate between AKI and CKD in MCQs?
Look for three key factors: timeline of creatinine rise (acute vs gradual), kidney size on imaging (normal vs small), and reversibility (AKI potentially reversible, CKD progressive). AKI shows recent creatinine elevation with normal-sized kidneys, while CKD shows gradual progression with small, scarred kidneys.
What is the best way to memorize electrolyte disorder ECG changes?
Use pattern recognition rather than memorization. Hypokalemia flattens everything (flat T waves, U waves), hyperkalemia peaks everything (peaked T waves, then widens QRS). Practice with actual ECG strips and connect the electrolyte physiology to the electrical changes you see.
Should I study pediatric and adult nephrology separately?
Study them together with age-specific variations. For example, learn glomerulonephritis principles first, then note that post-infectious GN and minimal change disease are more common in children while membranous nephropathy and FSGS predominate in adults. The pathophysiology remains similar across age groups.
How do I approach complex acid-base and electrolyte disorder MCQs?
Use a systematic approach: identify the primary disorder (metabolic vs respiratory acidosis/alkalosis), check for compensation, look for electrolyte abnormalities, and consider the clinical context. Practice mixed disorders frequently as NEET PG loves testing complex scenarios that combine multiple electrolyte disturbances.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for NEET PG. Download free on Android and iOS.