Back
Types of Vaccines and Vaccination Schedule India — MCQ Guide for NEET PG 2026
Master types of vaccines and UIP vaccination schedule for NEET PG 2026. Live vs killed vaccines, cold chain protocols, and high-yield MCQ facts with targeted practice.

Types of Vaccines and Vaccination Schedule India — MCQ Guide for NEET PG 2026
You are probably staring at another Community Medicine chapter thinking "vaccines again?" But here's the thing — NEET PG 2026 has been asking 8-12 vaccination MCQs every year, and they're not asking basic definitions anymore. They want mechanism-based questions about live vs killed vaccines, cold chain temperatures, and UIP schedule timelines that catch students off guard.
The questions have shifted. Instead of "Which vaccine is live?" you'll see "A 2-year-old missed MMR at 15 months. When can the next dose be given?" or "DPT vaccine stored at 8°C for 6 hours. What's the protocol?" These need instant recall of specific schedules and protocols.
This guide covers the high-yield vaccine types and UIP schedules that appear most frequently in NEET PG MCQs. We'll focus on classification systems, critical timelines, and the storage protocols that trip up students in the exam hall.
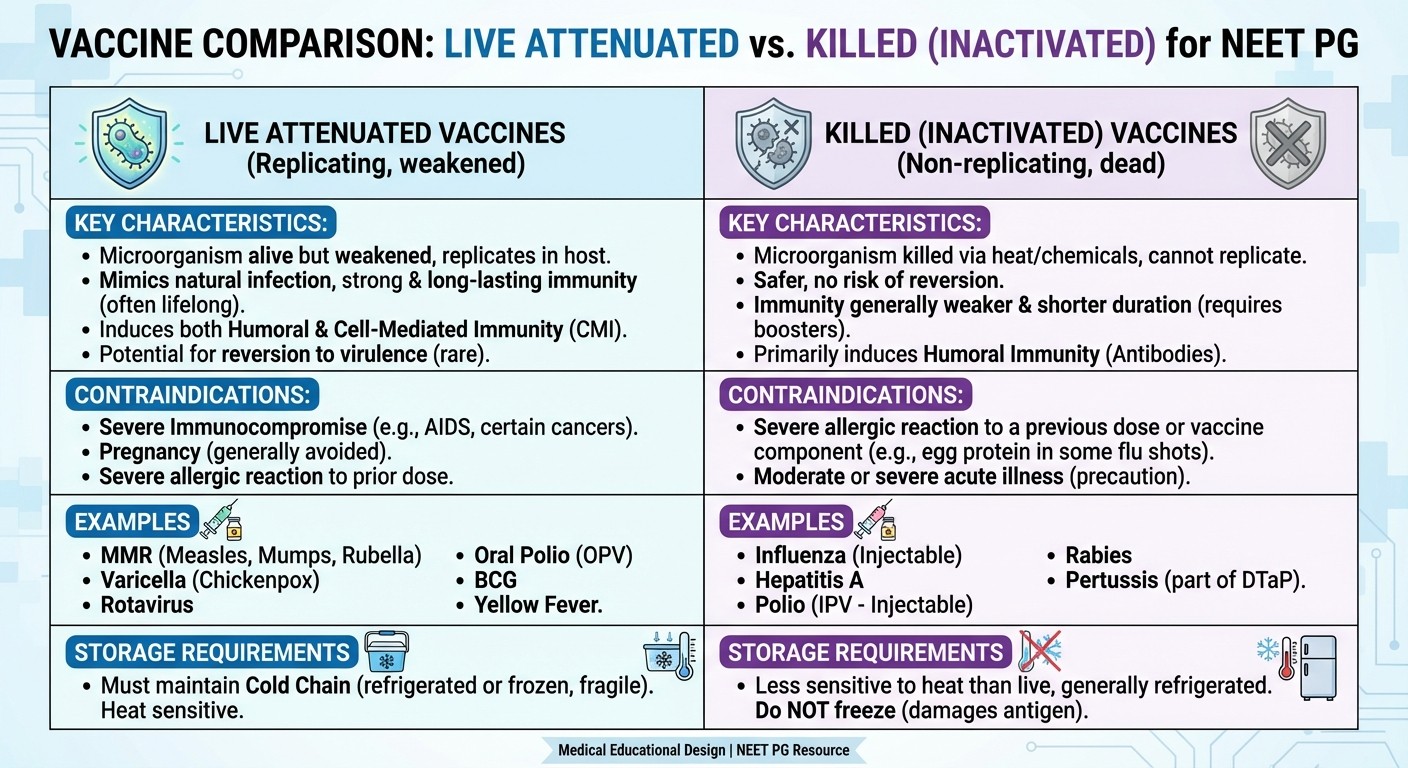
Live vs Killed Vaccines: The Classification That Matters
The live vs killed classification isnt just academic — it determines everything from storage requirements to contraindications to spacing between doses. NEET PG loves testing this distinction through clinical scenarios.
Live Attenuated Vaccines
These contain weakened but living organisms that replicate in the host. The key word here is "replicate" — this creates strong, long-lasting immunity but comes with specific risks and requirements.
Major live vaccines in UIP:
MMR (Measles, Mumps, Rubella)
OPV (Oral Polio Vaccine)
JE (Japanese Encephalitis) - live attenuated
Rotavirus vaccine
High-yield facts for MCQs:
Live vaccines require 4-week spacing if not given simultaneously
Contraindicated in immunocompromised patients
Can cause mild disease in recipients
Generally provide lifelong immunity
Cannot be given during pregnancy (except OPV in endemic areas)
The 4-week rule is heavily tested. If a child receives MMR today, any other live vaccine must wait 28 days. But killed vaccines? No waiting period needed.
Killed/Inactivated Vaccines
These contain dead organisms or purified components. They dont replicate, which means they're safer but require multiple doses for good immunity.
Major killed vaccines in UIP:
DPT (Diphtheria, Pertussis, Tetanus)
IPV (Inactivated Polio Vaccine)
Hepatitis B
Hib (Haemophilus influenzae type b)
PCV (Pneumococcal Conjugate Vaccine)
High-yield facts:
Safe in immunocompromised patients
Can be given during pregnancy when indicated
Require booster doses
No spacing required with other vaccines
Cannot cause disease from vaccination
Practice these distinctions with targeted vaccine MCQs that mirror actual NEET PG patterns.
Universal Immunization Program (UIP) Schedule 2026
The UIP schedule is the backbone of India's immunization strategy and appears in 15-20% of Community Medicine questions. You need to memorize specific ages and intervals — there's no partial credit for "around 6 months."
Birth Vaccines
Given within 24 hours:
BCG (0.1 ml intradermal, left upper arm)
OPV-0 (birth dose)
Hepatitis B-1 (0.5 ml intramuscular)
The 24-hour window is crucial for hepatitis B in preventing mother-to-child transmission. This timing appears frequently in MCQs about high-risk deliveries.
6-Week Schedule
At 6 weeks (earliest: 6 weeks, latest: 8 weeks):
DPT-1 (0.5 ml intramuscular, anterolateral thigh)
OPV-1
Hepatitis B-2
Hib-1
PCV-1 (introduced recently, often tested)
Rotavirus-1
The 6-week minimum age for DPT is non-negotiable — maternal antibodies interfere before this age. Questions often test early vaccination scenarios.
10-Week and 14-Week Follow-ups
10 weeks: DPT-2, OPV-2, Hib-2, PCV-2, Rotavirus-2 14 weeks: DPT-3, OPV-3, Hib-3, PCV-3, Rotavirus-3
The 4-week intervals between doses ensure proper immune response development. Shorter intervals reduce immunogenicity — a favorite MCQ trap.
Later Schedule Vaccines
9 months:
Measles-1 (0.5 ml subcutaneous)
JE-1 (in endemic areas)
12 months:
Hepatitis A (newly added to UIP)
15-18 months:
MMR (often confused with measles timing)
JE-2
DPT-4 (booster)
OPV-4 (booster)
24 months:
Measles-2 (campaign mode in some states)
Master these timelines with UIP schedule practice questions that test interval calculations and catch-up schedules.
Cold Chain Management: Temperature-Critical Details
Cold chain questions appear in every NEET PG, testing specific temperature ranges and equipment protocols. These arent approximate — you need exact numbers.
Temperature Requirements
Freeze-sensitive vaccines (2-8°C):
DPT, Hepatitis B, Hib, PCV
Never freeze — freezing destroys potency irreversibly
Freeze indicators used for monitoring
Freeze-tolerant vaccines (-15 to -25°C):
OPV, Measles, BCG
Can withstand freezing
Actually prefer frozen storage
Room temperature limits:
Most vaccines: maximum 30 minutes at room temperature
OPV: can stay out longer due to freeze tolerance
DPT: extremely sensitive to heat
Cold Chain Equipment
Walk-in cooler: +2 to +8°C, district level storage Ice-lined refrigerator (ILR): +2 to +8°C, PHC level Deep freezer: -15 to -25°C, ice pack preparation Vaccine carriers: maintain temperature for 2-3 days Cold boxes: larger capacity, 7-day maintenance
The 30-minute rule at room temperature is heavily tested. Questions often ask about vaccines left out during power cuts or transport delays.
Learn cold chain protocols systematically through dedicated cold chain lessons and practice questions.
Vaccine-Preventable Diseases: High-Yield Connections
NEET PG questions increasingly connect vaccine types to disease characteristics and epidemiology. Know which diseases each vaccine prevents and their clinical significance.
Bacterial Diseases
Diphtheria: Prevented by DPT, toxoid vaccine
Corynebacterium diphtheriae
Respiratory and cutaneous forms
Antitoxin treatment in cases
Pertussis: Prevented by DPT, whole cell or acellular
Bordetella pertussis
100-day cough in infants
Most severe in <6 months
Tetanus: Prevented by DPT and TT
Clostridium tetani
Wound contamination risk
Maternal immunization protects newborns
Viral Diseases
Polio: Prevented by OPV/IPV
Three serotypes of poliovirus
India declared polio-free 2014
AFP surveillance continues
Measles: Prevented by measles vaccine and MMR
Most contagious vaccine-preventable disease
Vitamin A deficiency increases severity
Complications: pneumonia, encephalitis
Hepatitis B: Prevented by hepatitis B vaccine
Chronic infection risk highest in infants
Birth dose prevents vertical transmission
High endemicity in India
Understanding disease burden helps you tackle MCQs about vaccine prioritization and program planning. Review vaccination coverage assessment to understand program effectiveness measures.
New Vaccines in UIP: Recent Updates for 2026
The UIP keeps expanding, and NEET PG tests knowledge of newly introduced vaccines. These questions catch students using outdated information.
Recently Added Vaccines
Pneumococcal Conjugate Vaccine (PCV):
Added to UIP in phases since 2017
Protects against Pneumococcus
3 doses: 6, 10, 14 weeks
Rotavirus Vaccine:
Prevents severe diarrhea in infants
Oral, live attenuated vaccine
3 doses with DPT schedule
Hepatitis A Vaccine:
Added at 12 months in some states
Single dose provides long protection
Reduces hepatitis A outbreaks
Measles-Rubella (MR) Vaccine:
Replacing standalone measles in campaigns
Part of rubella elimination strategy
Given in mass campaigns 9 months-15 years
Stay updated with new and underutilized vaccines content to avoid missing current program changes.
MCQ-High Yield Facts: What NEET PG Actually Tests
Based on recent NEET PG patterns, these facts appear most frequently in vaccine-related MCQs:
Timing and Intervals
6 weeks minimum: DPT, Hib, PCV, Rotavirus first dose
4 weeks spacing: Between doses of same vaccine series
28 days rule: Live vaccines if not given simultaneously
9 months earliest: Measles vaccine (maternal antibodies)
15-18 months: MMR timing (not same as measles)
Storage Protocols
2-8°C: DPT, Hepatitis B, Hib, PCV (freeze-sensitive)
-15 to -25°C: OPV, Measles, BCG (freeze-tolerant)
30 minutes max: Room temperature exposure for most vaccines
Freeze indicators: Monitor freeze-sensitive vaccines
Shake test: Check DPT for freezing damage
Contraindications
Live vaccines: Immunocompromised, pregnancy, severe illness
Killed vaccines: Severe illness only (safe in pregnancy/immunocompromised)
Egg allergy: Measles, MMR (grown in egg culture)
Previous reaction: Specific to that vaccine
Administrative Details
BCG site: Left upper arm, intradermal
DPT site: Anterolateral thigh, intramuscular
Measles site: Subcutaneous, any site
Dose volumes: 0.1 ml (BCG), 0.5 ml (most others)
These specifics cant be approximated during the exam. Use targeted vaccine flashcards for active recall of exact facts.
Special Vaccination Scenarios
NEET PG increasingly tests complex scenarios rather than straightforward schedule recall. These situational questions require deeper understanding of vaccination principles.
Immunocompromised Patients
Give: All killed vaccines (DPT, IPV, Hepatitis B, Hib, PCV)
Avoid: All live vaccines (MMR, OPV, measles, varicella)
Exception: Measles vaccine if CD4 >15% in HIV patients
Timing: Can give killed vaccines normally
Pregnancy Considerations
Safe in pregnancy: Tetanus toxoid, IPV (if indicated), Hepatitis B
Avoided in pregnancy: All live vaccines except OPV in endemic areas
Timing: Tetanus toxoid at 16 and 20 weeks for maternal immunization
Postpartum: Give any needed live vaccines immediately after delivery
Catch-up Schedules
Missed doses: Continue series, dont restart
Minimum intervals: 4 weeks for most vaccine series
Maximum age limits: DPT up to 7 years, then Td
Live vaccine spacing: 28 days if not simultaneous
Travel Vaccinations
JE vaccine: Live attenuated or killed, depending on formulation
Yellow fever: Live vaccine, contraindicated in pregnancy
Typhoid: Vi polysaccharide (killed) or Ty21a (live oral)
Documentation: International certificate requirements
Frequently Asked Questions
What's the difference between measles and MMR vaccine timing?
Measles vaccine is given at 9 months, while MMR is given at 15-18 months. This timing difference appears frequently in MCQs. The 9-month measles provides early protection, while MMR provides broader coverage including rubella.
Can live vaccines be given together?
Yes, live vaccines can be given simultaneously at different sites. If not given simultaneously, they must be spaced 4 weeks apart. This 28-day rule applies only to live vaccines — killed vaccines have no spacing requirements.
What happens if DPT is frozen accidentally?
Freezing destroys DPT vaccine irreversibly. The shake test can detect freezing damage — frozen DPT loses its fluffy appearance. Vaccine must be discarded and replaced.
How long can vaccines stay at room temperature?
Most vaccines can tolerate 30 minutes at room temperature. OPV can stay longer due to freeze tolerance. DPT and other freeze-sensitive vaccines are most vulnerable to heat damage.
What's the minimum age for first DPT dose?
6 weeks is the absolute minimum age for DPT-1. Giving earlier reduces immunogenicity due to maternal antibody interference. This timing is critical and heavily tested.
Which vaccines are contraindicated in pregnancy?
All live vaccines are contraindicated in pregnancy except OPV in endemic areas. Killed vaccines like tetanus toxoid and hepatitis B are safe when indicated.
Master Vaccine MCQs with Targeted Practice
Vaccination questions in NEET PG 2026 require precise recall of schedules, contraindications, and storage protocols. You cant approximate these facts during the exam — memorization through active practice is essential.
Review comprehensive immunization lessons and strengthen weak areas with spaced repetition flashcards. The systematic approach helps convert theoretical knowledge into instant MCQ recall.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for NEET PG success. Download free on Android and iOS.