Trauma/Emergencies US Medical PG Practice Questions and MCQs
Practice US Medical PG questions for Trauma/Emergencies. These multiple choice questions (MCQs) cover important concepts and help you prepare for your exams.
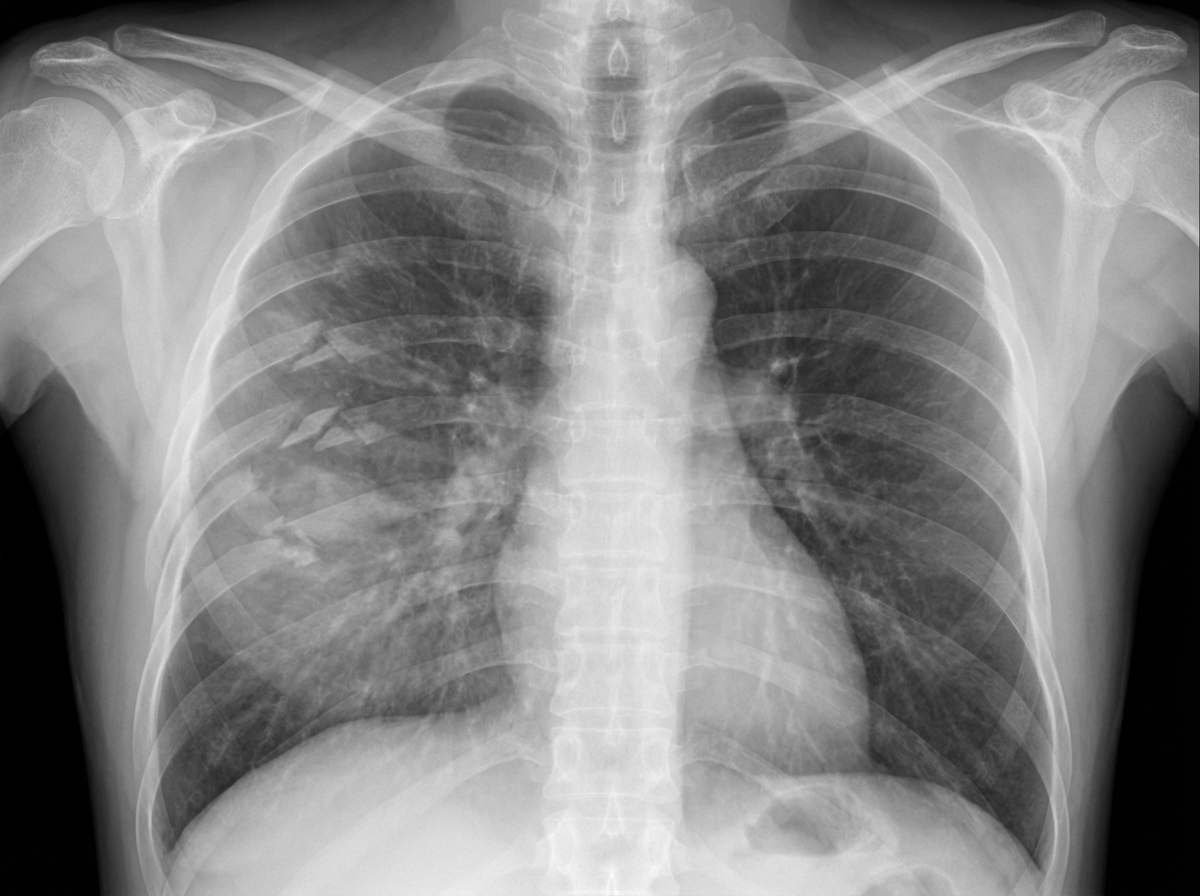
Trauma/Emergencies US Medical PG Question 1: A 27-year-old man is brought to the emergency department 45 minutes after being involved in a motor vehicle collision. He is agitated. He has pain in his upper right arm, which he is cradling in his left arm. His temperature is 36.7°C (98°F), pulse is 135/min, respirations are 25/min, and blood pressure is 145/90 mm Hg. His breathing is shallow. Pulse oximetry on 100% oxygen via a non-rebreather face mask shows an oxygen saturation of 83%. He is confused and oriented only to person. Examination shows multiple bruises on the right anterior thoracic wall. The pupils are equal and reactive to light. On inspiration, his right chest wall demonstrates paradoxical inward movement while his left chest wall is expanding. There is pain to palpation and crepitus over his right anterior ribs. The remainder of the examination shows no abnormalities. An x-ray of the chest is shown. Two large-bore IVs are placed. After fluid resuscitation and analgesia, which of the following is the most appropriate next step in management?
- A. Bedside thoracotomy
- B. Surgical fixation of right third to sixth ribs
- C. Intubation with positive pressure ventilation (Correct Answer)
- D. Placement of a chest tube
- E. CT scan of the chest
Trauma/Emergencies Explanation: ***Intubation with positive pressure ventilation***
- The patient presents with **flail chest** (paradoxical chest wall movement with pain and crepitus), respiratory distress (tachypnea, shallow breathing), and **hypoxemia** (SpO2 83% on 100% oxygen) despite initial fluid resuscitation and analgesia. These are clear indications for **endotracheal intubation** and mechanical ventilation to stabilize the chest wall, improve oxygenation, and reduce the work of breathing.
- **Positive pressure ventilation** helps to internally splint the flail segment, enabling more effective gas exchange and preventing further atelectasis.
*Bedside thoracotomy*
- **Bedside thoracotomy** is typically reserved for patients in traumatic cardiac arrest who have witnessed signs of life on arrival or are in profound shock unresponsive to other resuscitative measures, making it inappropriate here.
- This patient is **hemodynamically stable** (BP 145/90 mmHg) and does not show signs of massive hemorrhage or cardiac tamponade requiring immediate thoracotomy.
*Surgical fixation of right third to sixth ribs*
- **Surgical fixation of rib fractures** is a more definitive treatment for flail chest but is not an immediate life-saving intervention in the setting of acute respiratory failure and hypoxemia.
- While it can be considered later to reduce pain and improve pulmonary mechanics, the priority is to stabilize the patient's respiratory status through **ventilation**.
*Placement of a chest tube*
- **Placement of a chest tube** is indicated for pneumothorax, hemothorax, or empyema. While a pneumothorax or hemothorax could be present given the trauma and rib fractures, the primary issue driving this patient's acute respiratory failure is the **flail chest leading to inadequate ventilation and oxygenation**.
- There is no mention of diminished breath sounds or hyperresonance/dullness to percussion, which would suggest pneumothorax or hemothorax as the primary and immediate problem after initial resuscitation.
*CT scan of the chest*
- A **CT scan of the chest** is an important diagnostic tool to assess the extent of injuries, but it is not an immediate therapeutic intervention for a patient in acute respiratory failure and severe hypoxemia.
- Delaying definitive airway management for a diagnostic test in an unstable patient is **inappropriate** and could worsen the patient's condition.
Trauma/Emergencies US Medical PG Question 2: A 34-year-old man is admitted to the emergency department after a motor vehicle accident in which he sustained blunt abdominal trauma. On admission, he is conscious, has a GCS score of 15, and has normal ventilation with no signs of airway obstruction. Vitals initially are blood pressure 95/65 mmHg, heart rate 87/min, respiratory rate 14/min, and oxygen saturation of 95% on room air. The physical exam is significant only for tenderness to palpation over the left flank. Noncontrast CT of the abdomen shows fractures of the 9th and 10th left ribs. Intravenous fluids are administered and the patient's blood pressure increases to 110/80 mm Hg. Three days later after admission, the patient suddenly complains of weakness and left upper quadrant (LUQ) pain. Vitals are blood pressure 80/50 mm Hg, heart rate 97/min, respiratory rate 18/min, temperature 36.2℃ (97.2℉) and oxygen saturation of 99% on room air. Prompt administration of 2L of IV fluids increases the blood pressure to 100/70 mm Hg. On physical exam, there is dullness to percussion and rebound tenderness with guarding in the LUQ. Bowel sounds are present. Raising the patient's left leg results in pain in his left shoulder. Stat hemoglobin level is 9.8 g/dL. Which of the following findings would be most likely seen if a CT scan were performed now?
- A. Subdiaphragmatic air collection
- B. Low-density areas within the splenic parenchyma (Correct Answer)
- C. Heterogeneous parenchymal enhancement of the pancreatic tail
- D. Herniation of the stomach into the thoracic cavity
- E. Irregular linear areas of hypoattenuation in the liver parenchyma
Trauma/Emergencies Explanation: **Low-density areas within the splenic parenchyma**
- The patient's history of trauma, initial left rib fractures, LUQ pain, and **Kehr's sign** (left shoulder pain from diaphragmatic irritation), followed by sudden decompensation and anemia, are highly indicative of **delayed splenic rupture**.
- On CT scan, **low-density areas** (fluid collections or hematomas) within the splenic parenchyma or around the spleen are characteristic findings of splenic injury and rupture, including intraparenchymal hematomas or subcapsular hematomas.
*Subdiaphragmatic air collection*
- This finding suggests a **perforated viscus**, such as the stomach or intestine, allowing air to escape into the peritoneal cavity.
- While blunt trauma can cause hollow organ injury, the patient's symptoms (Kehr's sign, LUQ pain, initial rib fractures) and the delayed presentation of hypovolemic shock are more consistent with splenic rupture than perforation.
*Heterogeneous parenchymal enhancement of the pancreatic tail*
- This symptom is indicative of **pancreatic injury**, which can occur with blunt abdominal trauma, especially with rapid deceleration.
- However, the patient's presentation, particularly the prominent Kehr's sign and the context of left rib fractures, points more strongly towards splenic involvement rather than primary pancreatic injury.
*Herniation of the stomach into the thoracic cavity*
- This describes a **diaphragmatic rupture**, which can occur in severe blunt trauma and lead to gastric herniation.
- While possible with severe trauma, the immediate presentation of **Kehr's sign** and the progressive symptoms are more characteristic of splenic rupture than an acute diaphragmatic hernia with gastric displacement.
*Irregular linear areas of hypoattenuation in the liver parenchyma*
- These findings suggest **hepatic lacerations** or hematomas, indicating liver injury.
- Although liver injury is a common finding in blunt abdominal trauma, the patient's specific presentation of **left-sided pain**, **left shoulder pain**, and left rib fractures points preferentially to **splenic injury** rather than liver injury.
Trauma/Emergencies US Medical PG Question 3: A 3-year-old child is brought to the emergency department with multiple bruises in various stages of healing. X-rays reveal several metaphyseal fractures and posterior rib fractures. The parents claim the injuries resulted from normal play activities. Which of the following patterns would most strongly suggest non-accidental trauma?
- A. Circular bruises on the knees
- B. Loop-shaped bruises on the back (Correct Answer)
- C. Linear bruises on the shins
- D. Irregular bruises on the forehead
Trauma/Emergencies Explanation: ***Loop-shaped bruises on the back***
- **Loop-shaped bruises** are highly suspicious for **non-accidental trauma** as they are pathognomonic for impact with an object like a looped cord or belt
- Bruises on the **back** of a young child are particularly concerning as the back is a non-bony prominence and less likely to be injured during normal play activities
- Combined with the metaphyseal and posterior rib fractures already identified, patterned bruises strongly indicate inflicted trauma
*Circular bruises on the knees*
- Circular bruises on the knees are very common in toddlers and young children due to normal falls and play, which typically involve kneeling and crawling
- This pattern is generally considered consistent with accidental injury and not indicative of abuse
*Linear bruises on the shins*
- Linear bruises on the shins can result from bumping into objects while playing or exploring, which is common in active children
- The shins are bony prominences frequently injured during normal play activities
*Irregular bruises on the forehead*
- Irregular bruises on the forehead can result from accidental falls or bumps, which are common in young children learning to walk or play
- While head injuries should always be carefully evaluated, irregular bruises on the forehead are common accidental injuries in ambulatory toddlers
Trauma/Emergencies US Medical PG Question 4: A 35-year-old man is brought to the emergency department 20 minutes after being involved in a motor vehicle collision in which he was a restrained passenger. The patient is confused. His pulse is 140/min and blood pressure is 85/60 mm Hg. Examination shows a hand-sized hematoma on the anterior chest wall. An ECG shows sinus tachycardia. Which of the following structures is most likely injured in this patient?
- A. Papillary muscle
- B. Left main coronary artery
- C. Inferior vena cava
- D. Aortic isthmus (Correct Answer)
- E. Aortic valve
Trauma/Emergencies Explanation: ***Aortic isthmus***
- The **aortic isthmus** is the most common site of blunt **aortic injury** due to its relative immobility compared to the more mobile ascending aorta and arch. The deceleration forces experienced in a motor vehicle collision can cause a shearing injury at this location.
- The patient's **hypotension** and **tachycardia** are signs of significant hemorrhage, which is a common presentation of aortic injury. The chest wall hematoma also suggests significant trauma to the chest.
*Papillary muscle*
- Injury to the **papillary muscles** typically leads to severe **mitral regurgitation**, presenting with acute heart failure symptoms like pulmonary edema rather than primarily hypovolemic shock.
- While possible in trauma, the primary symptoms would involve a new significant murmur and rapid deterioration of cardiac function due to valve incompetence.
*Left main coronary artery*
- A **left main coronary artery** injury would likely lead to acute **myocardial ischemia** or infarction, manifesting as severe chest pain, ECG changes indicative of ischemia, and potentially cardiogenic shock, not hypovolemic shock.
- While trauma to the chest can cause coronary artery dissection, it is less common for blunt force to directly injure this artery without other, more widespread myocardial damage.
*Inferior vena cava*
- An injury to the **inferior vena cava (IVC)** would primarily cause severe internal bleeding, leading to hypovolemic shock. However, while possible, blunt force trauma to the chest is less likely to directly injure the retroperitoneal IVC without significant associated abdominal or lumbar spine injuries.
- The chest wall hematoma and focus on the chest suggests damage within the thoracic cavity, making an aortic injury more probable given the mechanism.
*Aortic valve*
- An injury to the **aortic valve** could cause acute **aortic regurgitation**, leading to acute heart failure and potentially cardiogenic shock with a new diastolic murmur.
- While possible, pure aortic valve injury from blunt trauma alone, without rupture of the aorta itself, is less common than aortic tear from shearing forces.
Trauma/Emergencies US Medical PG Question 5: A 28-year-old male presents to trauma surgery clinic after undergoing an exploratory laparotomy, femoral intramedullary nail, and femoral artery vascular repair 3 months ago. He suffered multiple gunshot wounds as a victim of a drive-by shooting. He is progressing well with well-healed surgical incisions on examination. He states during his clinic visit that he has been experiencing 6 weeks of nightmares where he "relives the day he was shot." The patient also endorses 6 weeks of flashbacks to "the shooter pointing the gun at him" during the daytime as well. He states that he has had difficulty sleeping and cannot concentrate when performing tasks. Which of the following is the most likely diagnosis?
- A. Schizophrenia
- B. Normal reaction to trauma
- C. Acute stress disorder
- D. Post-traumatic stress disorder (PTSD) (Correct Answer)
- E. Schizophreniform disorder
Trauma/Emergencies Explanation: ***Post-traumatic stress disorder (PTSD)***
- The patient's symptoms of **nightmares**, **flashbacks** (re-experiencing the trauma), **difficulty sleeping**, and **impaired concentration** following severe trauma are characteristic of PTSD.
- The symptoms have persisted for **6 weeks** (more than 1 month), meeting the duration criterion for PTSD diagnosis.
*Schizophrenia*
- Schizophrenia is characterized by **psychotic symptoms** such as hallucinations, delusions, and disorganized thought/speech, which are not described in this patient.
- While stress can exacerbate schizophrenia, the patient's symptoms are directly tied to a specific traumatic event, not a chronic psychotic disorder.
*Normal reaction to trauma*
- While some distress is expected after trauma, the presence of **persistent re-experiencing symptoms** (nightmares, flashbacks), and hyperarousal symptoms lasting for **over a month** is beyond a normal, transient reaction.
- These symptoms significantly impair the patient's functioning and indicate a clinically significant disorder.
*Acute stress disorder*
- Acute stress disorder presents with similar symptoms to PTSD, including intrusive thoughts, negative mood, dissociation, avoidance, and arousal.
- However, acute stress disorder is diagnosed when symptoms occur **3 days to 1 month** after trauma exposure; this patient's symptoms have lasted **6 weeks**, exceeding the 1-month threshold for ASD and meeting criteria for PTSD.
*Schizophreniform disorder*
- Schizophreniform disorder involves psychotic symptoms like **hallucinations, delusions, or disorganized speech**, lasting between 1 and 6 months.
- The patient's symptoms are primarily related to trauma re-experiencing and hyperarousal, not psychotic features.
More Trauma/Emergencies US Medical PG questions available in the OnCourse app. Practice MCQs, flashcards, and get detailed explanations.