Drug interactions and adverse effects US Medical PG Practice Questions and MCQs
Practice US Medical PG questions for Drug interactions and adverse effects. These multiple choice questions (MCQs) cover important concepts and help you prepare for your exams.
Drug interactions and adverse effects US Medical PG Question 1: A student is reviewing the various effects that can be plotted on a dose-response curve. He has observed that certain drugs can work as an agonist and an antagonist at a particular site. He has plotted a particular graph (as shown below) and is checking for other responses that can be measured on the same graph. He learned that drug B is less potent than drug A. Drug B also reduces the potency of drug A when combined in the same solution; however, if additional drug A is added to the solution, the maximal efficacy (Emax) of drug A increases. He wishes to plot another curve for drug C. He learns that drug C works on the same molecules as drugs A and B, but drug C reduces the maximal efficacy (Emax) of drug A significantly when combined with drug A. Which of the following best describes drug C?
- A. Reversible antagonist
- B. Competitive antagonist
- C. Full agonist
- D. Inverse agonist
- E. Non-competitive antagonist (Correct Answer)
Drug interactions and adverse effects Explanation: ***Non-competitive antagonist***
- A non-competitive antagonist **reduces the maximal efficacy (Emax)** of an agonist, even at high agonist concentrations. This is because it binds to a site other than the active site or binds irreversibly to the active site, preventing the agonist from producing its full effect.
- Unlike competitive antagonists, its effects cannot be overcome by simply increasing the concentration of the agonist.
*Reversible antagonist*
- This is a broad category; while some non-competitive antagonists can be reversible, the key characteristic for drug C is its impact on **maximal efficacy (Emax)**, which points more specifically to non-competitive antagonism.
- A reversible antagonist's effect can be overcome by increasing the agonist concentration, which is not the defining feature described for drug C.
*Competitive antagonist*
- A competitive antagonist **reduces the potency** (shifts the dose-response curve to the right, meaning a higher concentration of agonist is needed for the same effect) but **does not reduce the maximal efficacy (Emax)** of an agonist.
- Its effects can be fully overcome by adding more agonist, allowing the agonist to reach its original Emax.
*Full agonist*
- A full agonist **binds to a receptor and produces the maximal possible effect (Emax)**.
- This drug C is described as reducing the Emax of drug A, which is the opposite effect of an agonist.
*Inverse agonist*
- An inverse agonist **binds to a receptor and produces an effect opposite to that of a full agonist**, by stabilizing the receptor in an inactive conformation.
- While it modulates receptor activity, its primary action is not described as reducing the Emax of another agonist in the manner of an antagonist.
Drug interactions and adverse effects US Medical PG Question 2: A 61-year-old man with a history of type 1 diabetes mellitus and depression is brought to the emergency department because of increasing confusion and fever over the past 14 hours. Four days ago, he was prescribed metoclopramide by his physician for the treatment of diabetic gastroparesis. His other medications include insulin and paroxetine. His temperature is 39.9°C (103.8°F), pulse is 118/min, and blood pressure is 165/95 mm Hg. Physical examination shows profuse diaphoresis and flushed skin. There is generalized muscle rigidity and decreased deep tendon reflexes. His serum creatine kinase is 1250 U/L. Which of the following drugs is most likely to also cause this patient's current condition?
- A. Fluphenazine (Correct Answer)
- B. Tranylcypromine
- C. Desflurane
- D. Methamphetamine
- E. Nortriptyline
Drug interactions and adverse effects Explanation: **Fluphenazine**
- The patient's symptoms (fever, confusion, muscle rigidity, elevated CK, autonomic instability like tachycardia and hypertension) after starting metoclopramide are highly suggestive of **neuroleptic malignant syndrome (NMS)**. Metoclopramide is a **D2 receptor antagonist** that can precipitate NMS. Fluphenazine is a **typical antipsychotic** that also blocks D2 receptors and is a classic cause of NMS.
- The combination of **D2 receptor blockade** (by metoclopramide) and another potent D2 blocker like fluphenazine would significantly increase the risk of NMS.
*Tranylcypromine*
- This drug is a **monoamine oxidase inhibitor (MAOI)**. While it can cause **serotonin syndrome** when combined with serotonergic drugs like paroxetine, the clinical picture of NMS (marked rigidity, very high fever, elevated CK) is distinct from typical serotonin syndrome.
- Serotonin syndrome typically involves **hyperreflexia** and **clonus**, whereas this patient presents with **decreased deep tendon reflexes** and generalized **muscle rigidity**, key features of NMS.
*Desflurane*
- Desflurane is an **inhaled anesthetic** that can trigger **malignant hyperthermia** in susceptible individuals. Malignant hyperthermia shares some features with NMS (hyperthermia, muscle rigidity) but is specifically triggered by inhaled anesthetics and succinylcholine, not D2 antagonists.
- Malignant hyperthermia presents acutely during or immediately after anesthesia exposure, which is not consistent with the patient's presentation following metoclopramide initiation.
*Methamphetamine*
- Methamphetamine is a **stimulant** that can cause hyperthermia, tachycardia, and agitation. However, it does not typically cause the profound **muscle rigidity** and significantly elevated **creatine kinase** characteristic of NMS.
- The mechanism of action for methamphetamine is primarily related to increased release of dopamine, norepinephrine, and serotonin, not D2 receptor blockade leading to NMS.
*Nortriptyline*
- Nortriptyline is a **tricyclic antidepressant (TCA)**. While TCAs can have anticholinergic effects and cause some autonomic instability, they are not typically associated with NMS or malignant hyperthermia.
- Long-term use of TCAs can occasionally contribute to **serotonin syndrome** when combined with other serotonergic agents, but NMS is not a direct result.
Drug interactions and adverse effects US Medical PG Question 3: A 76-year-old man comes to the physician for a follow-up examination. One week ago, he was prescribed azithromycin for acute bacterial sinusitis. He has a history of atrial fibrillation treated with warfarin and metoprolol. Physical examination shows no abnormalities. Compared to one month ago, laboratory studies show a mild increase in INR. Which of the following best explains this patient's laboratory finding?
- A. Drug-induced hepatotoxicity
- B. Depletion of intestinal flora
- C. Inhibition of cytochrome p450 (Correct Answer)
- D. Increased gastrointestinal absorption of warfarin
- E. Increased non-protein bound warfarin fraction
Drug interactions and adverse effects Explanation: ***Inhibition of cytochrome p450***
- **Azithromycin**, while a weaker inhibitor compared to erythromycin and clarithromycin, **does inhibit CYP3A4 and other cytochrome P450 enzymes** to a clinically significant degree.
- This inhibition **reduces warfarin metabolism**, leading to increased warfarin levels and **enhanced anticoagulant effect**, manifesting as an **increased INR**.
- This pharmacokinetic interaction is well-documented and is the **primary mechanism** for azithromycin-warfarin interaction.
*Depletion of intestinal flora*
- The theory that antibiotics deplete **vitamin K-producing gut bacteria** leading to increased warfarin effect is a **common misconception**.
- Humans obtain vitamin K primarily from **dietary sources** (leafy greens, vegetable oils), not from gut bacterial synthesis; intestinal bacteria contribute minimally to vitamin K stores.
- This mechanism has been **debunked** in modern pharmacology literature and does not explain antibiotic-warfarin interactions.
*Drug-induced hepatotoxicity*
- While hepatotoxicity can impair **clotting factor synthesis** and increase INR, **azithromycin** rarely causes significant liver injury.
- The presentation shows only a **mild INR increase** one week after starting therapy, without other signs of liver dysfunction.
- This acute, mild change is more consistent with a **pharmacokinetic drug interaction** than hepatotoxicity.
*Increased gastrointestinal absorption of warfarin*
- **Warfarin** has high oral bioavailability (~100%) under normal conditions.
- **Azithromycin** does not enhance the **gastrointestinal absorption** of warfarin.
- This mechanism is not supported by pharmacological evidence for this drug interaction.
*Increased non-protein bound warfarin fraction*
- Displacement of warfarin from **plasma protein binding sites** can transiently increase free drug.
- However, **azithromycin** does not significantly displace warfarin from **albumin**.
- This mechanism does not explain the sustained INR elevation seen with azithromycin therapy.
Drug interactions and adverse effects US Medical PG Question 4: After being warned by the locals not to consume the freshwater, a group of American backpackers set off on a week-long hike into a region of the Ecuadorean Amazon forest known for large gold mines. The group of hikers stopped near a small stream and used the water they filtered from the stream to make dinner. Within the next half hour, the hikers began to experience headaches, vertigo, visual disturbances, confusion, tachycardia, and altered levels of consciousness. Which of the following enzymes was most likely inhibited in this group of hikers?
- A. NADH dehydrogenase
- B. ATP synthase
- C. Cytochrome c oxidase (Correct Answer)
- D. Cytochrome bc1 complex
- E. Succinate dehydrogenase
Drug interactions and adverse effects Explanation: ***Cytochrome c oxidase***
- The symptoms described (headaches, vertigo, visual disturbances, confusion, tachycardia, altered consciousness occurring within 30 minutes) are characteristic of **acute cyanide poisoning**.
- **Cyanide** is commonly found in water near **gold mining operations**, where it is used in the gold extraction process and can contaminate local water sources.
- **Cyanide** is a potent inhibitor of **cytochrome c oxidase** (Complex IV) in the electron transport chain, binding to the heme iron (Fe³⁺) and preventing oxygen utilization, leading to **histotoxic hypoxia**.
- This results in cellular energy failure, particularly affecting high-energy-demand organs like the brain and heart, explaining the acute neurological and cardiovascular symptoms.
*NADH dehydrogenase*
- While NADH dehydrogenase (Complex I) is a component of the electron transport chain, it is not the primary target of **cyanide poisoning**.
- Inhibitors of Complex I include rotenone and barbiturates, which cause different clinical presentations and do not produce the rapid onset of symptoms seen with cyanide.
*ATP synthase*
- **ATP synthase** (Complex V) synthesizes ATP using the proton gradient, but it is not directly inhibited by **cyanide**.
- Inhibitors of ATP synthase, such as oligomycin, prevent ATP synthesis by blocking the enzyme directly, whereas cyanide acts upstream at Complex IV.
*Cytochrome bc1 complex*
- The **cytochrome bc1 complex** (Complex III) is involved in electron transfer and proton pumping, but it is not the primary enzyme inhibited by **cyanide**.
- Inhibitors of Complex III include antimycin A, which would disrupt the electron transport chain but do not cause the characteristic rapid-onset symptoms of cyanide poisoning.
*Succinate dehydrogenase*
- **Succinate dehydrogenase** (Complex II) participates in both the citric acid cycle and the electron transport chain, but it is not targeted by **cyanide**.
- Inhibitors of Complex II, such as malonate, competitively block succinate oxidation but do not produce the acute systemic toxicity characteristic of cyanide poisoning.
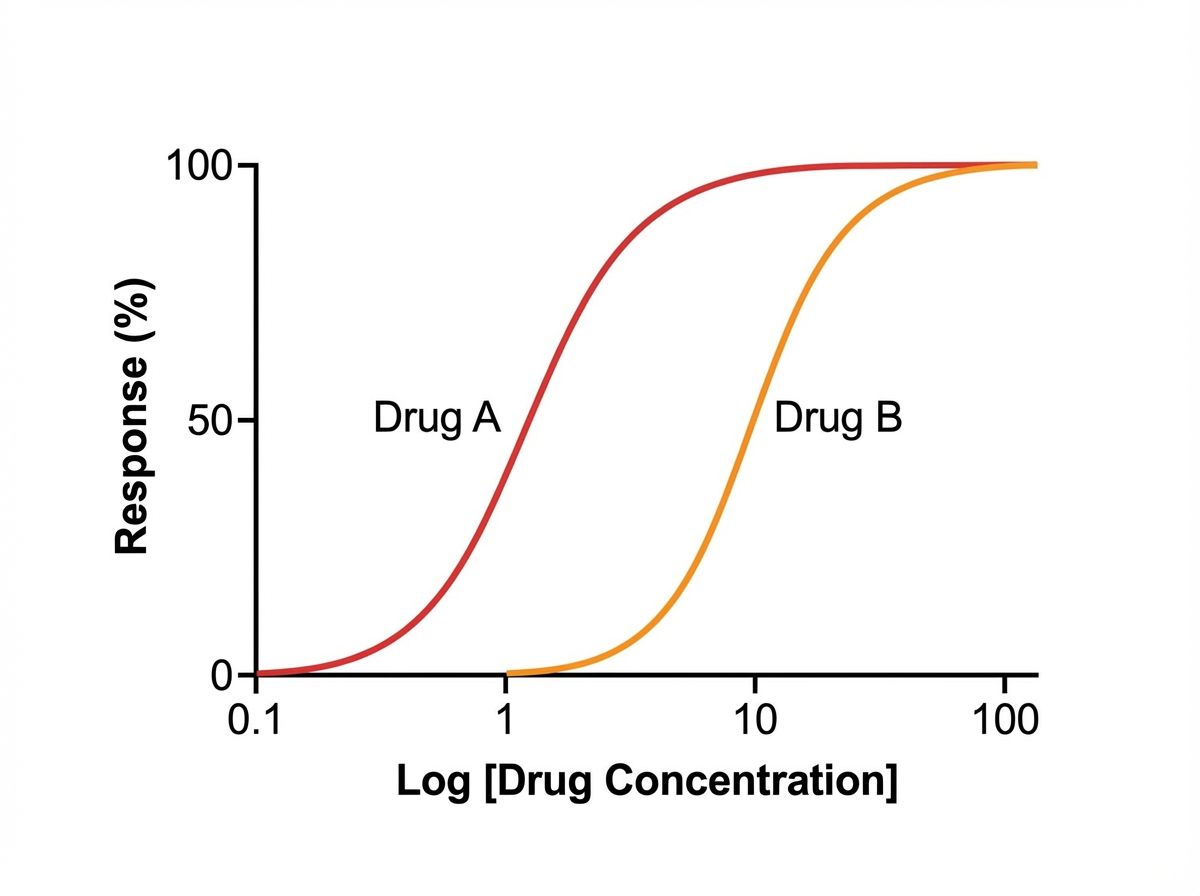
Drug interactions and adverse effects US Medical PG Question 5: A medical student is reviewing dose-response curves of various experimental drugs. She is specifically interested in the different factors that cause the curve to shift in different directions. From her study, she plots the following graph (see image). She marks the blue curve for drug A, which acts optimally on a receptor. After drawing the second (green) curve for drug B, she discovers that more of drug B is required to produce the same response as drug A, although drug B can still achieve the same maximum effect. Which of the following terms best describes the activity of drug B in comparison to drug A?
- A. Decreased efficacy
- B. Increased affinity
- C. Higher potency
- D. Higher efficacy
- E. Lower potency (Correct Answer)
Drug interactions and adverse effects Explanation: ***Lower potency***
- **Potency** refers to the amount of drug required to produce a given effect; if more of drug B is needed for the same response as drug A, it has lower potency.
- On a dose-response curve, **lower potency** is indicated by a rightward shift of the curve, meaning a higher dose is required to achieve any given effect.
*Decreased efficacy*
- **Efficacy** is the maximum effect a drug can produce, regardless of the dose.
- While drug B has a lower ability to produce a reaction (implying lower efficacy), the statement "more of the second drug B is required to produce the same response as the first one" specifically points to potency, not just the maximal effect.
*Increased affinity*
- **Affinity** describes how strongly a drug binds to its receptor.
- Increased affinity would generally lead to greater potency (less drug needed for an effect), which contradicts the scenario where more drug B is required.
*Higher potency*
- **Higher potency** would mean that less of drug B is required to produce the same effect as drug A, which is the opposite of what is described in the question.
- A drug with higher potency would cause the dose-response curve to shift to the left.
*Higher efficacy*
- **Higher efficacy** would mean drug B could produce a greater maximal effect than drug A, but the question states drug B has a "lower ability to produce a reaction" compared to drug A.
- The peak of the dose-response curve for drug B would be higher than drug A, which is not suggested by the description.
More Drug interactions and adverse effects US Medical PG questions available in the OnCourse app. Practice MCQs, flashcards, and get detailed explanations.