Common pediatric cancers US Medical PG Practice Questions and MCQs
Practice US Medical PG questions for Common pediatric cancers. These multiple choice questions (MCQs) cover important concepts and help you prepare for your exams.
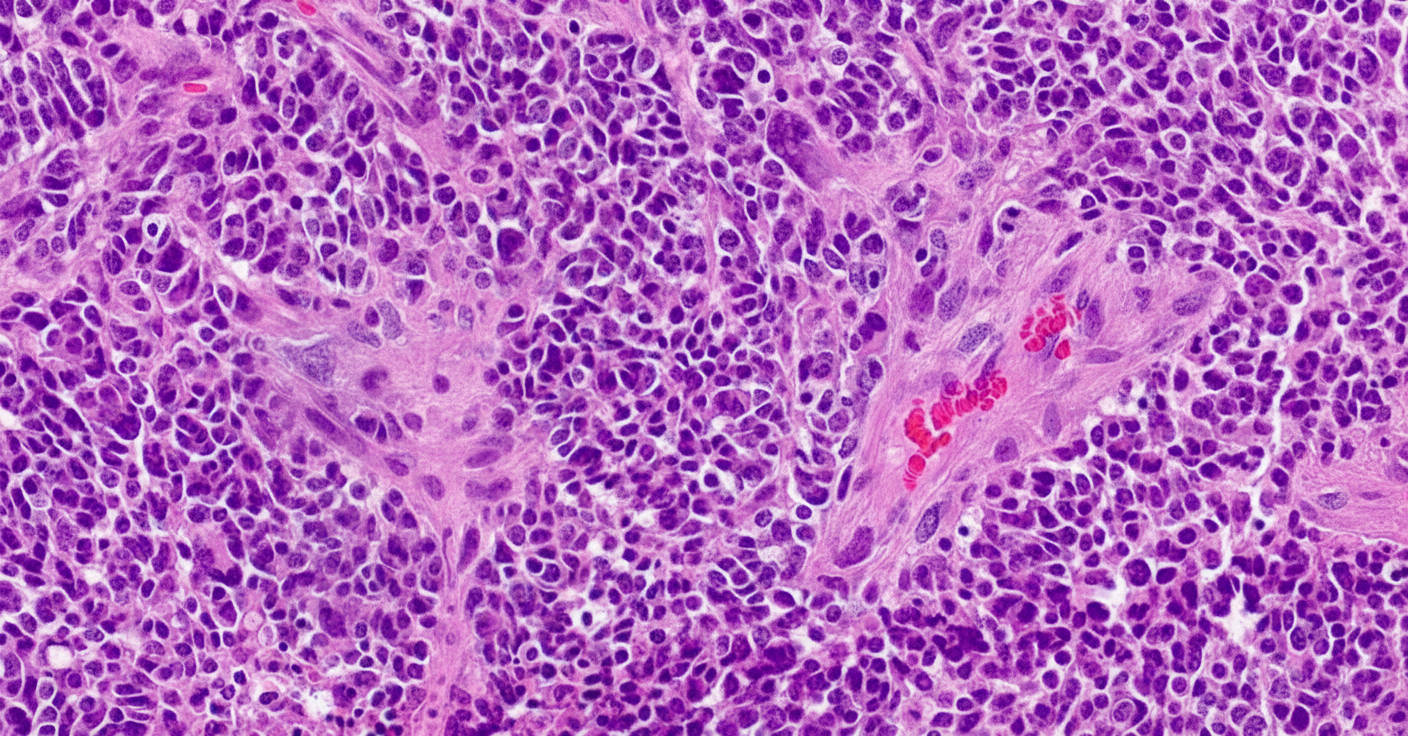
Common pediatric cancers US Medical PG Question 1: A previously healthy 4-year-old girl is brought to the physician for evaluation of a 3-week history of recurrent vomiting and difficulty walking. Examination shows a broad-based gait and bilateral optic disc swelling. An MRI shows an intracranial tumor. A ventriculoperitoneal shunt is placed, and surgical excision of the tumor is performed. A photomicrograph of a section of the tumor is shown. Which of the following is the most likely diagnosis?
- A. Medulloblastoma (Correct Answer)
- B. Hemangioblastoma
- C. Glioblastoma multiforme
- D. Oligodendroglioma
- E. Pinealoma
Common pediatric cancers Explanation: ***Medulloblastoma***
- This is the most common **malignant brain tumor** in children, typically arising in the **cerebellum** and presenting with **ataxia** (broad-based gait) and signs of **hydrocephalus** (vomiting, optic disc swelling) due to obstruction of CSF flow.
- Histologically, medulloblastomas are characterized by small, round blue cells with **high nuclear-to-cytoplasmic ratio**, often forming **Homer-Wright rosettes**, indicating their primitive neuroectodermal origin.
*Hemangioblastoma*
- These are typically **benign tumors** of vascular origin, most commonly found in the **cerebellum** of adults and associated with **von Hippel-Lindau disease**.
- Histologically, they consist of foamy stromal cells and a dense capillary network, which is distinct from the provided image.
*Glioblastoma multiforme*
- This is the most common and aggressive primary brain tumor in **adults**, primarily affecting the cerebral hemispheres.
- Histologically, it is characterized by **astrocytic cells** with pleomorphism, high mitotic activity, **necrosis** with pseudopalisading, and vascular proliferation, which is not depicted in the image.
*Oligodendroglioma*
- These are typically found in the **cerebral hemispheres** of adults and are characterized by a **"fried egg"** appearance due to perinuclear halos and a capillary network with a **"chicken wire"** pattern.
- Their incidence in children is much lower, and the presented image is not consistent with this histology.
*Pinealoma*
- Tumors of the **pineal gland** can occur in children but often present with symptoms related to compression of the tectum (**Parinaud syndrome**) or hydrocephalus due to aqueductal compression.
- The most common pineal tumor is a **germinoma**, which has a different histological appearance (large round cells with prominent nucleoli amidst a lymphocytic infiltrate).
Common pediatric cancers US Medical PG Question 2: A 12-month-old girl is brought to her pediatrician for a checkup and vaccines. The patient’s mother wants to send her to daycare but is worried about exposure to unvaccinated children and other potential sources of infection. The toddler was born at 39 weeks gestation via spontaneous vaginal delivery. She is up to date on all vaccines. She does not walk yet but stands in place and can say a few words. The toddler drinks formula and eats a mixture of soft vegetables and pureed meals. She has no current medications. On physical exam, the vital signs include: temperature 37.0°C (98.6°F), blood pressure 95/50 mm Hg, pulse 130/min, and respiratory rate 28/min. The patient is alert and responsive. The remainder of the exam is unremarkable. Which of the following is most appropriate for this patient at this visit?
- A. Meningococcal vaccine
- B. Gross motor workup and evaluation
- C. Rotavirus vaccine
- D. Referral for speech pathology
- E. MMR vaccine (Correct Answer)
Common pediatric cancers Explanation: ***MMR vaccine***
- The **measles, mumps, and rubella (MMR) vaccine** is recommended for administration at **12-15 months of age**.
- This timing offers protection against these common childhood diseases, which is especially important for children attending **daycare**.
*Meningococcal vaccine*
- The routine **meningococcal vaccine (MenACWY)** is typically recommended for adolescents at **11-12 years of age**, with a booster at 16 years.
- While there are specific circumstances for earlier vaccination (e.g., high-risk conditions), it is **not routine** for a 12-month-old.
*Gross motor workup and evaluation*
- The patient's motor development, standing in place but not yet walking, is **within the normal range** for a 12-month-old.
- A definitive **gross motor workup** would generally be considered if there were more significant delays or regressions.
*Rotavirus vaccine*
- The **rotavirus vaccine** series is typically given at **2, 4, and 6 months of age**, with the final dose administered no later than **8 months of age**.
- A 12-month-old is **outside the recommended age range** for initiating or completing this vaccine series.
*Referral for speech pathology*
- Saying "a few words" at 12 months is **within the normal developmental milestone** for expressive language at this age.
- A referral for **speech pathology** would generally be indicated for more significant language delays.
Common pediatric cancers US Medical PG Question 3: A 3-year-old male child is found to have a disease involving DNA repair. Specifically, he is found to have a defect in the endonucleases involved in the nucleotide excision repair of pyrimidine dimers. Which of the following is a unique late-stage complication of this child's disease?
- A. Telangiectasia
- B. Colorectal cancer
- C. Malignant melanoma (Correct Answer)
- D. Lymphomas
- E. Endometrial cancer
Common pediatric cancers Explanation: **Malignant melanoma**
- The described condition is **xeroderma pigmentosum**, an autosomal recessive disorder characterized by a defect in **nucleotide excision repair (NER)**, specifically the inability to remove **pyrimidine dimers** caused by **UV radiation**.
- This severely impaired DNA repair leads to an extreme predisposition to **UV-induced skin cancers**, including basal cell carcinomas, squamous cell carcinomas, and, most aggressively, **malignant melanoma**, which is a unique and life-threatening late-stage complication.
*Telangiectasia*
- **Telangiectasias** are dilated small blood vessels that appear on the skin or mucous membranes and can be associated with various conditions.
- While skin abnormalities are prevalent in xeroderma pigmentosum due to sun damage, **melanoma** is a more specific and severe late-stage complication directly resulting from the DNA repair defect.
*Colorectal cancer*
- **Colorectal cancer** is typically associated with other DNA repair defects, such as those in the **mismatch repair system**, as seen in conditions like **Lynch syndrome**.
- It is not a primary or most significant late-stage complication of xeroderma pigmentosum, which is primarily characterized by skin cancers.
*Lymphomas*
- **Lymphomas** are cancers of the lymphatic system, often linked to immune deficiencies or specific genetic translocations.
- While individuals with genetic syndromes can have increased cancer risks, **lymphoma** is not the hallmark late-stage complication of xeroderma pigmentosum; skin cancers are the predominant concern.
*Endometrial cancer*
- **Endometrial cancer** is a gynecological cancer often associated with hormonal factors or genetic predispositions like Lynch syndrome, which involves mismatch repair defects.
- This type of cancer is not a characteristic or unique late-stage complication of xeroderma pigmentosum, whose pathology is centered on **UV-induced DNA damage** and subsequent skin malignancies.
Common pediatric cancers US Medical PG Question 4: A 4-year-old girl is being followed by the pediatric oncology team after her pediatrician found a palpable abdominal mass towards the right flank 2 weeks ago. Abdominal ultrasonography detected a solid mass in the right kidney without infiltration of the renal vein and inferior vena cava. The contrast-enhanced computed tomography (CT) confirmed the presence of a solitary mass in the right kidney surrounded by a pseudocapsule consisting of a rim of normal tissue, displacing it medially, and distorting the collecting system. No nodal involvement was detected. In which of the following chromosomes would you expect a genetic abnormality?
- A. Chromosome 13
- B. Chromosome 1
- C. Chromosome 3
- D. Chromosome 22
- E. Chromosome 11 (Correct Answer)
Common pediatric cancers Explanation: ***Chromosome 11***
- This clinical presentation, particularly the **solitary renal mass** in a 4-year-old and the imaging findings of a **pseudocapsule** and displacement of the collecting system, is highly suggestive of **Wilms tumor (nephroblastoma)**.
- **Wilms tumor** is associated with genetic abnormalities, most notably mutations in the **WT1 gene** located on **chromosome 11p13**, and the **WT2 locus** on **chromosome 11p15.5**.
*Chromosome 13*
- Abnormalities on **chromosome 13** are primarily associated with **retinoblastoma**, linked to mutations in the **RB1 gene**.
- While retinoblastoma is a childhood cancer, its presentation involves ocular tumors, not renal masses.
*Chromosome 1*
- Genetic abnormalities on **chromosome 1** are implicated in various cancers and conditions, but they are not the primary or most characteristic genetic defect associated with **Wilms tumor**.
- Specific translocations or deletions on chromosome 1 can be seen in certain leukemias and lymphomas, which do not fit the clinical picture.
*Chromosome 3*
- **Chromosome 3** abnormalities are well-known in various malignancies, most notably **renal cell carcinoma (RCC)**, particularly the **von Hippel-Lindau (VHL) gene** at 3p25-26.
- RCC is typically a cancer of adulthood, and VHL disease presents with multiple organ system involvement, differing from a solitary renal mass in a young child.
*Chromosome 22*
- Abnormalities on **chromosome 22** are frequently associated with conditions like **neurofibromatosis type 2** (NF2 gene) and **DiGeorge syndrome** (22q11 deletion).
- The presentation of a renal mass in a child is not characteristic of genetic defects on chromosome 22.
Common pediatric cancers US Medical PG Question 5: A 5-year-old boy presents to his pediatrician with weakness. His father observed that his son seemed less energetic at daycare and kindergarten classes. He was becoming easily fatigued from mild play. His temperature is 98°F (37°C), blood pressure is 90/60 mmHg, pulse is 100/min, and respirations are 20/min. Physical exam reveals pale conjunctiva, poor skin turgor and capillary refill, and cervical and axillary lymphadenopathy with assorted bruises throughout his body. A complete blood count reveals the following:
Leukocyte count: 3,000/mm^3
Segmented neutrophils: 30%
Bands: 5%
Eosinophils: 5%
Basophils: 10%
Lymphocytes: 40%
Monocytes: 10%
Hemoglobin: 7.1 g/dL
Hematocrit: 22%
Platelet count: 50,000/mm^3
The most specific diagnostic assessment would most likely show which of the following?
- A. Bone marrow biopsy with ≥ 20% lymphoblasts (Correct Answer)
- B. Fluorescence in situ hybridization analysis with 9:22 translocation
- C. Peripheral blood smear with > 50% lymphoblasts
- D. Flow cytometry with positive terminal deoxynucleotidyl transferase staining
- E. Fluorescence in situ hybridization analysis with 12:21 translocation
Common pediatric cancers Explanation: ***Bone marrow biopsy with ≥ 20% lymphoblasts***
- The patient's symptoms (weakness, fatigue, pallor, bruising, lymphadenopathy) and blood counts (anemia, thrombocytopenia, leukopenia with relative lymphocytosis) are highly suggestive of **Acute Lymphoblastic Leukemia (ALL)**.
- The most specific diagnostic assessment for ALL involves a **bone marrow biopsy** showing **≥20% lymphoblasts** per WHO 2016 classification, confirming the abnormal proliferation of immature lymphoid cells.
- This is the **gold standard** for diagnosing ALL and distinguishes it from other hematologic disorders.
*Fluorescence in situ hybridization analysis with 9:22 translocation*
- The **Philadelphia chromosome (t[9;22])** is characteristic of **Chronic Myeloid Leukemia (CML)**, which is rare in children and presents differently.
- While t(9;22) can occur in 3-5% of childhood ALL and indicates poor prognosis, it is a **prognostic marker**, not the primary diagnostic criterion for ALL itself.
*Peripheral blood smear with > 50% lymphoblasts*
- While lymphoblasts can be seen in the peripheral blood in ALL, a specific percentage threshold in peripheral blood is **not a diagnostic criterion** for ALL.
- The peripheral blood smear can be suggestive, but the **bone marrow blast percentage is the gold standard** for definitive diagnosis.
*Flow cytometry with positive terminal deoxynucleotidyl transferase staining*
- **Terminal deoxynucleotidyl transferase (TdT)** is a nuclear enzyme expressed in pre-B and pre-T lymphoblasts and is an important marker for ALL.
- Flow cytometry with positive TdT staining helps **characterize and classify the blasts** but does not quantify the blast percentage required for diagnosis, which is provided by the bone marrow biopsy.
*Fluorescence in situ hybridization analysis with 12:21 translocation*
- The **t(12;21) [ETV6-RUNX1] translocation** is the most common cytogenetic abnormality in childhood B-cell ALL (20-25% of cases) and is associated with favorable prognosis.
- While its presence is relevant for risk stratification and treatment planning, the primary diagnostic criterion for ALL is the **percentage of lymphoblasts in the bone marrow**.
More Common pediatric cancers US Medical PG questions available in the OnCourse app. Practice MCQs, flashcards, and get detailed explanations.