Cell injury US Medical PG Practice Questions and MCQs
Practice US Medical PG questions for Cell injury. These multiple choice questions (MCQs) cover important concepts and help you prepare for your exams.
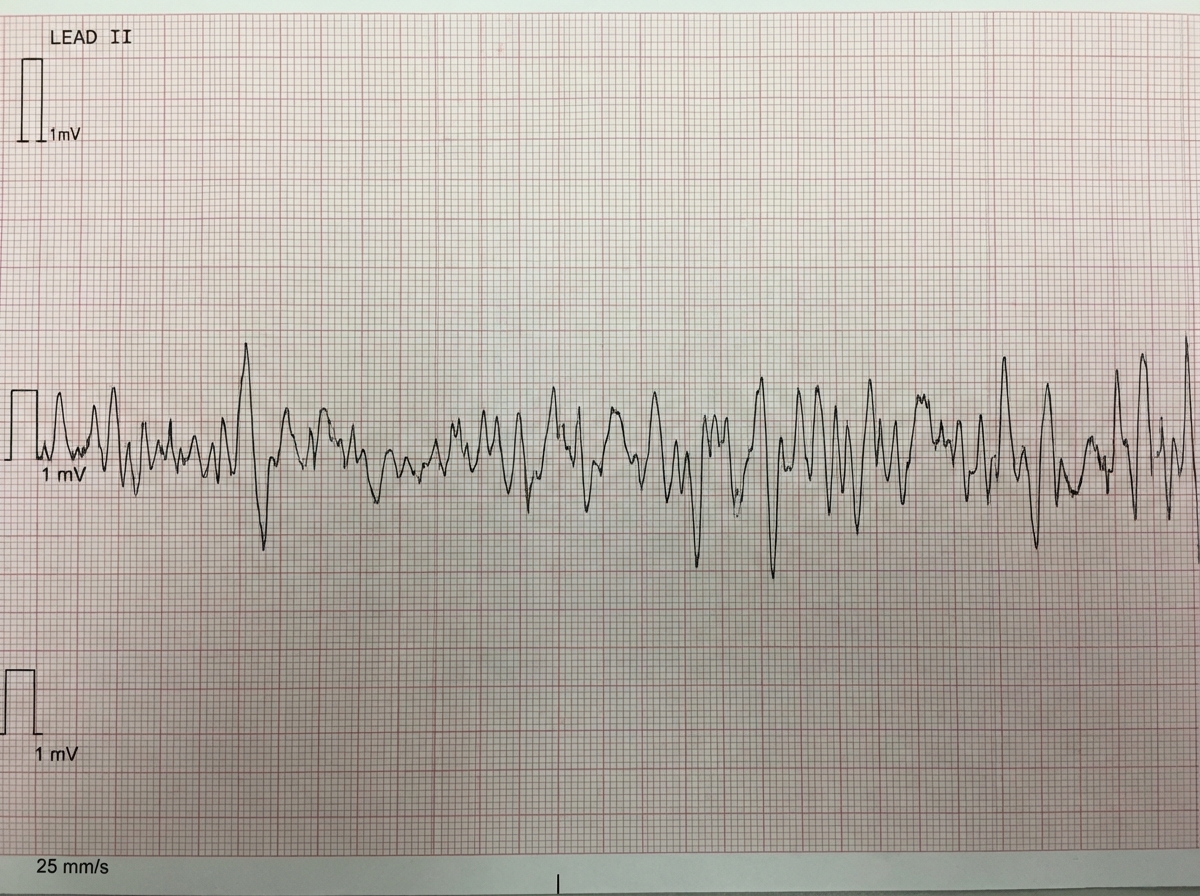
Cell injury US Medical PG Question 1: One hour after being admitted to the hospital for sharp, acute chest pain and diaphoresis, a 55-year-old woman with type 2 diabetes mellitus loses consciousness in the emergency department. There are no palpable pulses. Chest compressions are started. The patient has a history of breast cancer that was surgically treated 4 years ago. Prior to admission, the patient was on a long bus ride to visit her sister. Her medications include tamoxifen, atorvastatin, metoprolol, metformin, and insulin. Serum troponin levels are elevated. The cardiac rhythm is shown. Which of the following is the most appropriate next step in management?
- A. Defibrillation (Correct Answer)
- B. Coronary angiography
- C. Intravenous dextrose therapy
- D. Intravenous epinephrine therapy
- E. Intravenous glucagon therapy
Cell injury Explanation: ***Defibrillation***
- The ECG shows **ventricular fibrillation (VF)**, characterized by chaotic, disorganized electrical activity with no identifiable QRS complexes and no palpable pulse. VF is a **shockable rhythm**.
- According to ACLS guidelines, the immediate management for VF is **unsynchronized defibrillation** along with high-quality chest compressions.
- Defibrillation depolarizes the myocardium simultaneously, allowing the sinoatrial node to potentially resume normal electrical activity and restore organized cardiac rhythm.
- For refractory VF after initial shocks, epinephrine and antiarrhythmics (amiodarone or lidocaine) are added.
*Intravenous epinephrine therapy*
- Epinephrine is a vasopressor used in cardiac arrest to increase coronary and cerebral perfusion pressure.
- While epinephrine is given during VF arrest, it is administered **after** the initial defibrillation attempts, not as the immediate first step.
- Epinephrine is the primary drug for **non-shockable rhythms** (PEA and asystole), but defibrillation takes priority in shockable rhythms like VF.
*Intravenous glucagon therapy*
- Glucagon is used for severe **hypoglycemia** or **beta-blocker/calcium channel blocker overdose**.
- While the patient takes metoprolol (a beta-blocker), the clinical presentation with elevated troponin, chest pain, and VF rhythm clearly indicates an acute cardiac event, not beta-blocker toxicity.
- Glucagon has no role in the immediate management of cardiac arrest from VF.
*Coronary angiography*
- Coronary angiography is indicated for **post-cardiac arrest care** after return of spontaneous circulation (ROSC), especially in patients with suspected acute coronary syndrome.
- The patient has elevated troponin suggesting acute MI, making early angiography important **after** successful resuscitation.
- However, angiography cannot be performed during active cardiac arrest; immediate defibrillation and CPR are required first.
*Intravenous dextrose therapy*
- Dextrose is used to treat **hypoglycemia**.
- While the patient has diabetes and takes insulin (hypoglycemia risk), the presentation with chest pain, elevated troponin, and VF rhythm indicates acute coronary syndrome with cardiac arrest.
- Hypoglycemia does not cause VF; the rhythm is consistent with ischemic cardiac arrest requiring immediate defibrillation.
Cell injury US Medical PG Question 2: Which transport mechanism is primarily responsible for calcium reabsorption in the proximal tubule?
- A. Paracellular transport (Correct Answer)
- B. Facilitated diffusion
- C. Active transport
- D. Antiport with sodium
Cell injury Explanation: ***Paracellular transport***
- In the **proximal tubule**, approximately 60-70% of filtered calcium is reabsorbed primarily through the **paracellular pathway**, driven by the electrochemical gradient and solvent drag.
- This transport occurs between cells, moving through the **tight junctions**, and is passive, following the reabsorption of water.
*Facilitated diffusion*
- While a type of passive transport, **facilitated diffusion** typically involves membrane proteins and occurs across the cell membrane, not primarily between cells in the proximal tubule for calcium.
- This mechanism is prominent for calcium reabsorption in other nephron segments like the **distal convoluted tubule** via **TRPV5/6 channels**, but not the main route in the proximal tubule.
*Active transport*
- **Active transport** of calcium, mainly via **calcium ATPase** and the **Na+/Ca2+ exchanger**, occurs across the luminal and basolateral membranes, respectively, in specific nephron segments.
- However, in the **proximal tubule**, the bulk of calcium reabsorption is passive and paracellular, not ATP-dependent active transport across cell membranes.
*Antiport with sodium*
- The **Na+/Ca2+ exchanger (NCX)** is an antiport mechanism that plays a crucial role in extruding calcium from the cell into the interstitium, particularly in the basolateral membrane of the distal tubule.
- However, it is not the primary mechanism for overall tubular reabsorption of calcium in the **proximal tubule**, where paracellular movement dominates.
Cell injury US Medical PG Question 3: A 52-year-old man is brought to the emergency department by ambulance after a motor vehicle accident. He was an unrestrained passenger who was ejected from the vehicle. On presentation, he is found to be actively bleeding from numerous wounds. His blood pressure is 76/42 mmHg and pulse is 152/min. Attempts at resuscitation fail, and he dies 25 minutes later. Autopsy shows blood in the peritoneal cavity, and histology of the kidney reveals swelling of the proximal convoluted tubule epithelial cells. Which of the following is most likely the mechanism underlying the renal cell findings?
- A. Decreased activity of caspase 7
- B. Increased activity of caspase 9
- C. Increased function of the Na+/K+-ATPase
- D. Increased activity of caspase 8
- E. Decreased function of the Na+/K+-ATPase (Correct Answer)
Cell injury Explanation: ***Decreased function of the Na+/K+-ATPase***
- The patient experienced **hypovolemic shock** due to severe blood loss, leading to a significant drop in blood pressure and organ perfusion. This results in **ischemia** of the renal cells.
- **Ischemic injury** impairs ATP production, which is essential for the function of the **Na+/K+-ATPase pump**. Failure of this pump leads to intracellular accumulation of sodium and water, causing **cellular swelling**, particularly noticeable in the proximal convoluted tubules.
*Decreased activity of caspase 7*
- **Caspases**, including caspase 7, are involved in **apoptosis** (programmed cell death), which involves cell shrinkage and fragmentation, not the swelling observed here.
- Decreased caspase activity would generally *reduce* apoptosis, which is not the primary mechanism of acute cell injury in shock.
*Increased activity of caspase 9*
- Increased activity of **caspase 9** is indicative of the **intrinsic apoptotic pathway**, typically initiated by mitochondrial damage.
- While prolonged ischemia can eventually lead to apoptotic changes, the acute finding of **cellular swelling** points more directly to immediate membrane pump dysfunction due to ATP depletion.
*Increased function of the Na+/K+-ATPase*
- **Increased function** of the Na+/K+-ATPase would actively pump sodium out of the cell and potassium in, *preventing* intracellular swelling.
- This option contradicts the observed finding of proximal convoluted tubule epithelial cell swelling, which is characteristic of acute cellular injury due to pump failure.
*Increased activity of caspase 8*
- **Caspase 8** is a key initiator caspase in the **extrinsic apoptotic pathway**, often triggered by death receptor signaling.
- Similar to caspase 9, increased caspase 8 activity would lead to apoptosis, characterized by cell shrinkage, not the **cellular swelling** seen in acute ischemic injury.
Cell injury US Medical PG Question 4: An investigator is examining tissue samples from various muscle tissue throughout the body. She notices that biopsies collected from a specific site have a high concentration of sarcoplasmic reticulum, mitochondria, and myoglobin; they also stain poorly for ATPase. Additionally, the cell surface membranes of the myocytes in the specimen lack voltage-gated calcium channels. These myocytes are found in the greatest concentration at which of the following sites?
- A. Ventricular myocardium
- B. Tunica media
- C. Lateral rectus muscle
- D. Glandular myoepithelium
- E. Semispinalis muscle (Correct Answer)
Cell injury Explanation: ***Semispinalis muscle***
- The described characteristics—**high concentration of sarcoplasmic reticulum, mitochondria, and myoglobin** with **poor ATPase staining**—are hallmarks of **Type I (slow-twitch oxidative) skeletal muscle fibers**.
- Postural muscles like the **semispinalis** (part of the erector spinae group) are predominantly composed of Type I fibers adapted for sustained, aerobic contraction to maintain posture.
- These fibers appear **red** due to high myoglobin content, have abundant mitochondria for aerobic metabolism, and stain **poorly for ATPase** (distinguishing them from Type II fast-twitch fibers).
- While all skeletal muscle does possess voltage-gated calcium channels for excitation-contraction coupling, the overall profile best matches slow-twitch postural muscles.
*Ventricular myocardium*
- While cardiac muscle has high mitochondria, myoglobin, and sarcoplasmic reticulum, it **does possess L-type voltage-gated calcium channels** on the sarcolemma, which are essential for cardiac excitation-contraction coupling.
- Cardiac muscle relies on **both** extracellular Ca²⁺ influx through these channels and calcium-induced calcium release from the SR.
- Cardiac muscle typically stains **strongly for ATPase**, not poorly.
*Tunica media*
- Composed of **vascular smooth muscle** with poorly developed sarcoplasmic reticulum and relatively few mitochondria compared to skeletal or cardiac muscle.
- Smooth muscle relies heavily on **extracellular calcium influx** and the calmodulin pathway for contraction.
- Not characterized by high myoglobin content.
*Lateral rectus muscle*
- This extraocular muscle contains predominantly **Type IIb fast-twitch glycolytic fibers** adapted for rapid, precise eye movements.
- These fibers have **low myoglobin** (white muscle), fewer mitochondria, and stain **strongly for ATPase**.
- Opposite profile from the described tissue.
*Glandular myoepithelium*
- Myoepithelial cells are specialized contractile cells in secretory glands with minimal sarcoplasmic reticulum and mitochondria.
- Function is brief contraction for secretion expulsion, not sustained aerobic work.
- Do not exhibit the high oxidative capacity described.
Cell injury US Medical PG Question 5: A 72-year-old man presents to the emergency department after a fall. The patient was found lying down on the floor in his room in his retirement community. The patient has a past medical history of Alzheimer dementia and a prosthetic valve. His current medications include donepezil and warfarin. His temperature is 97.7°F (36.5°C), blood pressure is 85/50 mmHg, pulse is 160/min, respirations are 13/min, and oxygen saturation is 97% on room air. The patient is started on IV fluids and a type and screen is performed. Laboratory values are ordered as seen below.
Hemoglobin: 13 g/dL
Hematocrit: 39%
Leukocyte count: 5,500 cells/mm^3 with normal differential
Platelet count: 225,000/mm^3
INR: 2.5
AST: 10 U/L
ALT: 12 U/L
A chest radiograph and EKG are performed and are within normal limits. A full physical exam is within normal limits. The patient's vitals are repeated. His temperature is 99.5°F (37.5°C), blood pressure is 110/70 mmHg, pulse is 90/min, respirations are 10/min, and oxygen saturation is 98% on room air. Which of the following is the best next step in management?
- A. CT scan (Correct Answer)
- B. Urgent blood transfusion
- C. Fresh frozen plasma
- D. Exploratory laparoscopy
- E. Exploratory laparotomy
Cell injury Explanation: ***CT scan***
- A patient with a **prosthetic valve** on **warfarin** and a fall is at high risk for **intracranial hemorrhage**, even without focal neurological deficits.
- While initial vitals improved after IV fluids, the mechanism of injury (fall) and medication profile warrant a **CT scan** of the head to rule out serious internal injury, especially given the history of dementia which might mask symptoms.
*Urgent blood transfusion*
- The patient's **hemoglobin (13 g/dL)** and **hematocrit (39%)** are within normal limits, indicating no acute need for blood transfusion due to hemorrhage.
- Transfusions are typically reserved for patients with significant blood loss or severe symptomatic anemia.
*Fresh frozen plasma*
- The patient's **INR of 2.5** is within the therapeutic range for a patient with a prosthetic valve on warfarin.
- There is no evidence of active bleeding or supratherapeutic anticoagulation that would necessitate the administration of **fresh frozen plasma (FFP)** to reverse anticoagulation.
*Exploratory laparoscopy*
- There are no clinical signs or symptoms, such as abdominal pain, distension, or evidence of intra-abdominal bleeding (e.g., declining hemoglobin, peritoneal signs), to suggest an indication for an **exploratory laparoscopy**.
- The patient's physical exam was described as normal.
*Exploratory laparotomy*
- Similar to laparoscopy, there is no clinical evidence of acute abdominal injury or hemorrhage, which would necessitate an **exploratory laparotomy**.
- This invasive procedure is reserved for cases with strong suspicion of significant intra-abdominal pathology or trauma.
More Cell injury US Medical PG questions available in the OnCourse app. Practice MCQs, flashcards, and get detailed explanations.