Stages of labor US Medical PG Practice Questions and MCQs
Practice US Medical PG questions for Stages of labor. These multiple choice questions (MCQs) cover important concepts and help you prepare for your exams.
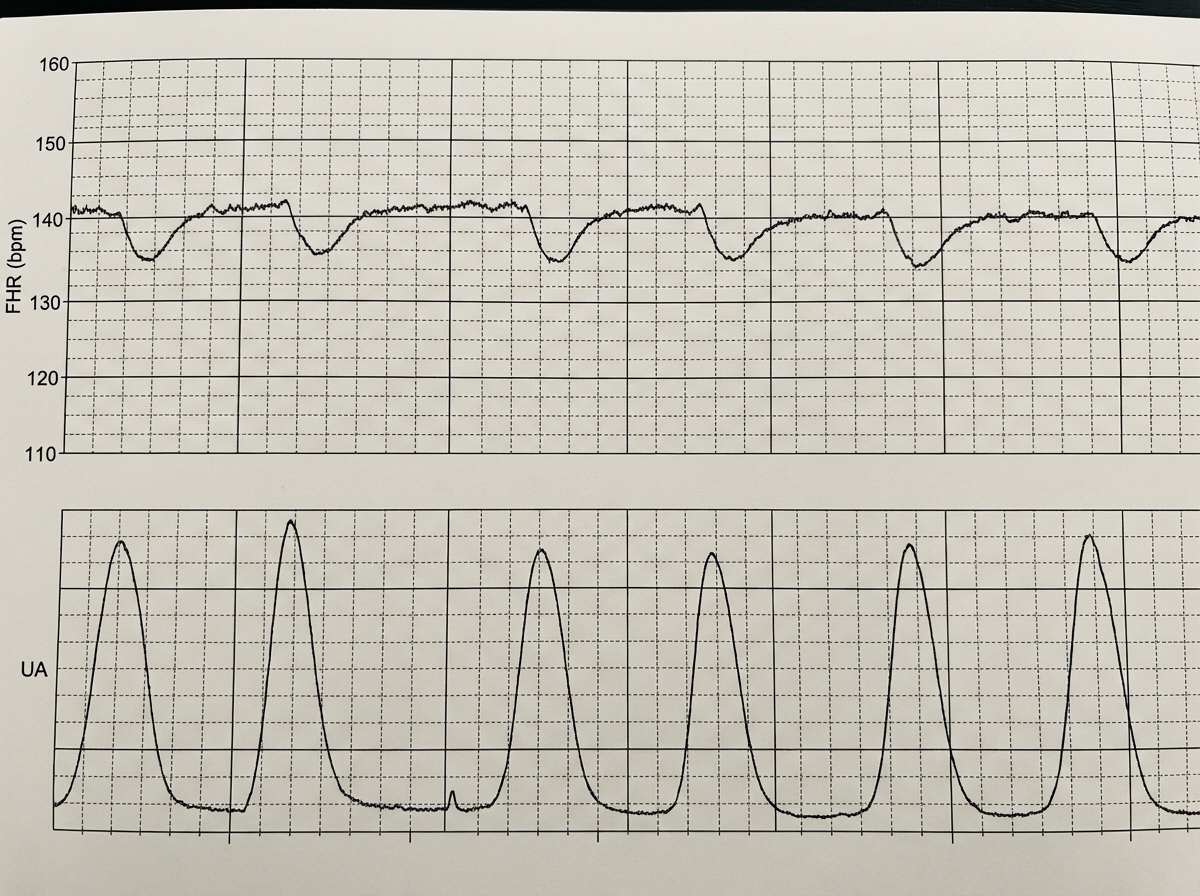
Stages of labor US Medical PG Question 1: A 39-year-old woman, gravida 5, para 4, at 41 weeks' gestation is brought to the hospital because of regular uterine contractions that started 2 hours ago. Pregnancy has been complicated by iron deficiency anemia treated with iron supplements. Pelvic examination shows the cervix is 90% effaced and 7-cm dilated; the vertex is at -1 station. Fetal heart tracing is shown. The patient is repositioned, O2 therapy is initiated, and amnioinfusion is done. A repeat assessment after 20 minutes shows a similar cervical status, and no changes in the fetal heart tracing, and less than 5 contractions in a period of 10 minutes.What is the most appropriate next step in management?
- A. Emergent cesarean delivery (Correct Answer)
- B. Monitor without intervention
- C. Begin active pushing
- D. Retry maternal repositioning
- E. Administer tocolytics
Stages of labor Explanation: ***Emergent cesarean delivery***
- The fetal heart tracing shows **recurrent late decelerations** unresponsive to **intrauterine resuscitation** (repositioning, O2, amnioinfusion), indicating fetal distress and uteroplacental insufficiency.
- Given the fetal distress and persistent late decelerations despite interventions, **expedited delivery** via cesarean section is indicated to prevent further fetal compromise.
*Monitor without intervention*
- This approach is inappropriate as the fetal heart tracing indicates **fetal distress** with recurrent **late decelerations** that have not resolved with initial interventions.
- Continued monitoring without action would place the fetus at risk for **hypoxia** and acidosis.
*Begin active pushing*
- The cervix is 7-cm dilated, meaning the patient is still in the **active phase of labor** and has not reached **complete cervical dilation** (10 cm) necessary for effective pushing.
- Pushing at this stage is unlikely to resolve the fetal distress and can potentially worsen **fetal acidosis** and maternal exhaustion.
*Retry maternal repositioning*
- The patient has already been repositioned and received other intrauterine resuscitation measures (O2 therapy, amnioinfusion) without improvement in the fetal heart tracing.
- Repeated repositioning alone is unlikely to resolve the underlying cause of the **late decelerations** in this context.
*Administer tocolytics*
- Tocolytics are used to **reduce uterine contractions** and manage conditions like **uterine tachysystole** or arrested labor, which are not explicitly present as the primary problem here (less than 5 contractions in 10 minutes).
- While they can temporarily improve uterine blood flow, they do not address the persistent **fetal distress** indicated by the recurrent late decelerations unresponsive to other interventions.
Stages of labor US Medical PG Question 2: Two days after vaginal delivery of a healthy newborn at term, a 32-year-old woman, gravida 2, para 2, is unable to breastfeed. Her labor was complicated by antepartum hemorrhage and she received two units of packed red blood cells. Her pulse is 99/min and blood pressure is 90/55 mm Hg. Further evaluation of this patient is most likely to show which of the following sets of serum findings?
$$$ ACTH %%% Aldosterone %%% Cortisol $$$
- A. ↑ ↓ ↓
- B. ↓ ↑ ↓
- C. ↑ normal ↑
- D. ↓ normal ↑
- E. ↓ normal ↓ (Correct Answer)
Stages of labor Explanation: ***↓ normal ↓***
- This scenario describes **Sheehan's syndrome**, caused by **postpartum pituitary necrosis** due to severe hemorrhage and hypotension during delivery.
- Decreased **ACTH** (adrenocorticotropic hormone) leads to secondary **adrenal insufficiency**, causing decreased **cortisol**. **Aldosterone** secretion, primarily regulated by the **renin-angiotensin system**, remains largely normal because only the zona glomerulosa of the adrenal cortex, which produces aldosterone, is regulated directly by the renin-angiotensin-aldosterone system (RAAS), whereas the pituitary regulates the zona fasciculata and zona reticularis.
*↑ ↓ ↓*
- This pattern (high ACTH, low aldosterone, low cortisol) suggests **primary adrenal insufficiency** (Addison's disease), where the adrenal glands themselves are failing, leading to a compensatory increase in ACTH. However, this patient's condition is due to pituitary damage.
- In primary adrenal insufficiency, both **cortisol** and **aldosterone** would be low, and **ACTH** would be elevated due to a lack of negative feedback.
*↓ ↑ ↓*
- This pattern (low ACTH, high aldosterone, low cortisol) is inconsistent with most common adrenal or pituitary pathologies. Low ACTH and low cortisol would suggest secondary adrenal insufficiency, but high aldosterone does not fit.
- **Hyperaldosteronism** with secondary adrenal insufficiency is rare and not indicated by the patient's presentation.
*↑ normal ↑*
- This pattern (high ACTH, normal aldosterone, high cortisol) suggests **Cushing's disease** (pituitary adenoma secreting ACTH), or an ectopic ACTH tumor, or a state of acute stress.
- The patient's **hypotension** and inability to breastfeed point away from Cushing's and towards hypopituitarism.
*↓ normal ↑*
- This pattern (low ACTH, normal aldosterone, high cortisol) could be seen in states of iatrogenic **exogenous corticosteroid use**, leading to suppressed ACTH and endogenous cortisol, or in an adrenal tumor producing cortisol independent of ACTH.
- This is inconsistent with the symptoms of postpartum hemorrhage and inability to lactate, which indicate a **deficit** rather than an excess of pituitary hormones.
Stages of labor US Medical PG Question 3: A 29-year-old G1P0 female at 32 weeks gestation presents to the emergency department with vaginal bleeding. She has had minimal prenatal care to-date with only an initial visit with an obstetrician after a positive home pregnancy test. She describes minimal spotting that she noticed earlier today that has progressed to larger amounts of blood; she estimates 30 mL of blood loss. She denies any cramping, pain, or contractions, and she reports feeling continued movements of the baby. Ultrasound and fetal heart rate monitoring confirm the presence of a healthy fetus without any evidence of current or impending complications. The consulted obstetrician orders blood testing for Rh-status of both the mother as well as the father, who brought the patient to the hospital. Which of the following represents the best management strategy for this situation?
- A. After 28 weeks gestation, administration of RhoGAM will have no benefit
- B. If mother is Rh-positive and father is Rh-negative then administer RhoGAM
- C. If mother is Rh-negative and father is Rh-negative then administer RhoGAM
- D. If mother is Rh-negative and father is Rh-positive, RhoGAM administration is not needed
- E. If mother is Rh-negative and father is Rh-positive then administer RhoGAM (Correct Answer)
Stages of labor Explanation: ***If mother is Rh-negative and father is Rh-positive then administer RhoGAM***
- This combination creates a risk for **Rh incompatibility**, meaning the fetus could be Rh-positive and the mother's immune system could form antibodies against fetal red blood cells, which can harm the fetus in future pregnancies.
- **RhoGAM (Rh immunoglobulin)** administration prevents the mother from forming these antibodies when there's a risk of maternal-fetal blood mixing, as indicated by vaginal bleeding.
*After 28 weeks gestation, administration of RhoGAM will have no benefit*
- This statement is incorrect; **RhoGAM is routinely administered around 28 weeks gestation** as prophylaxis in Rh-negative mothers, even without bleeding episodes, to prevent sensitization.
- In cases of potential fetal-maternal hemorrhage, such as vaginal bleeding, RhoGAM is indicated regardless of gestational age beyond the first trimester.
*If mother is Rh-positive and father is Rh-negative then administer RhoGAM*
- This scenario does not pose a risk for **Rh incompatibility hemolytic disease of the newborn**, as the mother already possesses the Rh antigen.
- RhoGAM is specifically given to Rh-negative mothers to prevent their immune system from reacting to an Rh-positive fetus.
*If mother is Rh-negative and father is Rh-negative then administer RhoGAM*
- In this case, both parents are **Rh-negative**, meaning the fetus will also be Rh-negative.
- There is no risk of **Rh incompatibility** or sensitization, so RhoGAM administration is not indicated.
*If mother is Rh-negative and father is Rh-positive, RhoGAM administration is not needed*
- This statement is incorrect and represents a critical misunderstanding of **Rh incompatibility prophylaxis**.
- This specific genetic combination creates the highest risk for **Rh sensitization** during pregnancy, especially with events like vaginal bleeding, making RhoGAM administration essential.
Stages of labor US Medical PG Question 4: A 28-year-old primigravid woman at 36 weeks' gestation comes to the emergency department for 2 hours of contractions. Her pregnancy has been uncomplicated. The contractions occur once every 20–30 minutes, last less than 30 seconds, and have been consistent in intensity and duration since onset. During that time there has been an increase in fetal movements. Her temperature is 37.1°C (98.8°F), pulse is 98/min, and blood pressure is 104/76 mm Hg. Pelvic examination shows clear cervical mucus and a firm uterus consistent in size with a 36-week gestation. The cervix is 0% effaced and undilated; the vertex is at -3 station. The fetal heart rate is reassuring. After an hour of monitoring in the emergency department, the character of the contractions and pelvic examination findings remain unchanged. Which of the following is the most appropriate next step?
- A. Admit for continuous monitoring
- B. Reassurance and discharge (Correct Answer)
- C. Administer tocolytics
- D. Perform cesarean delivery
- E. Offer local or regional anesthesia
Stages of labor Explanation: ***Reassurance and discharge***
- The patient's symptoms (contractions every 20-30 minutes, lasting less than 30 seconds, consistent in intensity and duration, **no cervical changes**) are consistent with **Braxton Hicks contractions** rather than true labor.
- Given the reassuring fetal movements, normal vital signs, and unchanged cervical examination after an hour of monitoring, **reassurance and discharge** with instructions to return for signs of true labor are appropriate.
*Admit for continuous monitoring*
- Admission for continuous monitoring is indicated for **true labor**, suspected fetal distress, or complications requiring close observation.
- This patient's findings, including lack of cervical change and stable contraction pattern, do not meet criteria for admission.
*Administer tocolytics*
- **Tocolytics** are used to stop or slow down premature labor.
- This patient is at **36 weeks' gestation** (near term) and is not in true labor, making tocolytic administration inappropriate and unnecessary.
*Perform cesarean delivery*
- **Cesarean delivery** is indicated for obstetric emergencies, fetal distress, or failed vaginal delivery.
- There are no indications for an operative delivery at this time; the patient is not in active labor and both mother and fetus are stable.
*Offer local or regional anesthesia*
- **Local or regional anesthesia** (e.g., epidural) is typically offered for pain management during active labor.
- Since the patient is not in active labor, pain management for labor is not necessary.
Stages of labor US Medical PG Question 5: A 22-year-old primigravid woman at 41 weeks' gestation is admitted to the hospital in active labor. Pregnancy has been uncomplicated. She has asthma treated with theophylline and inhaled corticosteroids. She has had 2 surgeries in the past to repair multiple lower limb and pelvis fractures that were the result of a car accident. She is otherwise healthy. Her temperature is 37.2°C (99°F) and blood pressure is 108/70 mm Hg. Examination shows the cervix is 100% effaced and 10 cm dilated; the vertex is at -4 station, with the occiput in the anterior position. Uterine activity is measured at 275 MVUs. Maternal pushing occurs during the contractions. Fetal heart tracing is 166/min and reactive with no decelerations. Epidural anesthesia is initiated for pain relief. After 4 hours of pushing, the vertex is found to be at -4 station, with increasing strength and rate of uterine contractions; fetal heart tracing shows late decelerations. Which of the following is the most likely cause of this patient's prolonged labor?
- A. Deep transverse arrest
- B. Insufficient uterine contraction
- C. Epidural anesthesia
- D. Cephalopelvic disproportion (Correct Answer)
- E. Inefficient maternal pushing
Stages of labor Explanation: ***Cephalopelvic disproportion***
- The history of **multiple lower limb and pelvis fractures** from a car accident suggests a high likelihood of a **contracted or abnormally shaped pelvis**. This can lead to **cephalopelvic disproportion (CPD)**, where the fetal head cannot fit through the maternal pelvis despite adequate uterine contractions (275 MVUs).
- The combination of **prolonged labor** (4 hours of pushing with no descent), **vertex at -4 station** even after full dilation, increasing contraction strength, and new **late decelerations** (indicating fetal distress due to impaired oxygenation from prolonged compression) points towards an obstruction.
*Deep transverse arrest*
- This occurs when the fetal head rotates into the transverse diameter of the pelvis and fails to rotate anteriorly. While it causes **arrest of descent and dilation**, the primary issue is **malposition**, not a fundamental size mismatch.
- The occiput is described as in the **anterior position**, which does not immediately suggest deep transverse arrest.
*Insufficient uterine contraction*
- The uterine activity is measured at **275 MVUs**, which indicates **adequate contraction strength**. Insufficient contractions would typically be below 200 MVUs.
- While weak contractions can cause prolonged labor, the current uterine activity suggests this is not the primary problem.
*Epidural anesthesia*
- Epidural anesthesia can sometimes prolong the second stage of labor by reducing the urge to push or temporarily decreasing the effectiveness of pushing efforts. However, the patient's **strong uterine activity (275 MVUs)** and previous **pelvic fractures** make a mechanical obstruction (CPD) a more specific and likely cause of arrest in this scenario.
- Furthermore, the vertex remaining at -4 station for 4 hours despite strong contractions points to a physical barrier rather than just altered pushing dynamics.
*Inefficient maternal pushing*
- While inefficient maternal pushing can contribute to prolonged labor, the fetus remaining at -4 station for 4 hours with **strong uterine contractions (275 MVUs)** indicates that the issue is likely beyond just inadequate pushing efforts.
- The historical detail of **pelvic fractures** points more strongly to an anatomical obstruction rather than simply ineffective maternal exertion.
More Stages of labor US Medical PG questions available in the OnCourse app. Practice MCQs, flashcards, and get detailed explanations.