Stroke US Medical PG Practice Questions and MCQs
Practice US Medical PG questions for Stroke. These multiple choice questions (MCQs) cover important concepts and help you prepare for your exams.
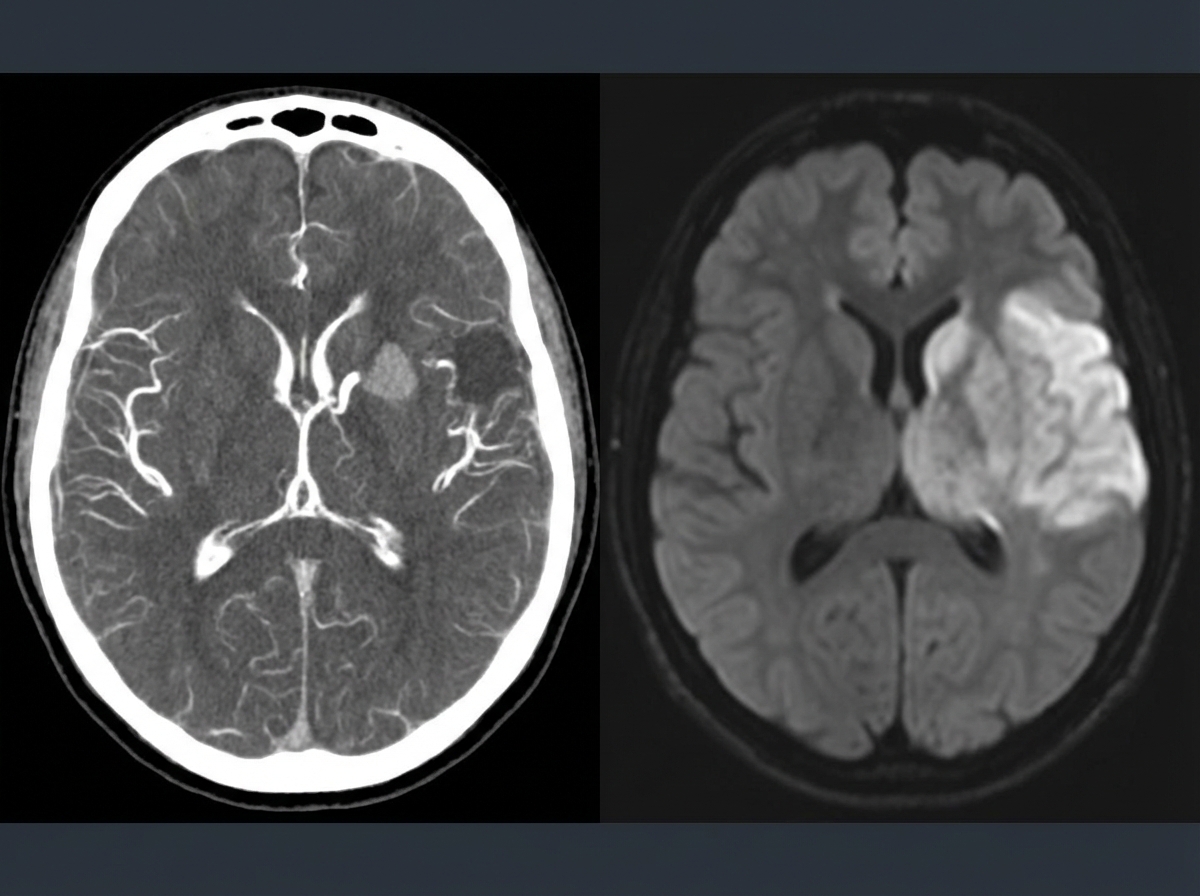
Stroke US Medical PG Question 1: A 69-year-old man is brought in by his wife with acute onset aphasia for the past 5 hours. The patient's wife says that they were sitting having dinner when suddenly he was not able to speak. They delayed coming to the hospital because he had a similar episode 2 months ago which resolved within an hour. His past medical history is significant for hypercholesterolemia, managed with rosuvastatin, and a myocardial infarction (MI) 2 months ago, status post percutaneous transluminal coronary angioplasty complicated by residual angina. His family history is significant for his father who died of MI at age 60. The patient reports a 15-pack-year smoking history but denies any alcohol or recreational drug use. The vital signs include: temperature 37.0℃ (98.6℉), blood pressure 125/85 mm Hg, pulse 96/min, and respiratory rate 19/min. On physical examination, the patient has expressive aphasia. There is a weakness of the right-sided lower facial muscles. The strength in his upper and lower extremities is 4/5 on the right and 5/5 on the left. There is also a decreased sensation on his right side. A noncontrast computed tomography (CT) scan of the head is unremarkable. CT angiography (CTA) and diffusion-weighted magnetic resonance imaging (MRI) of the brain are acquired, and the findings are shown in the exhibit (see image). Which of the following is the best course of treatment in this patient?
- A. Aspirin
- B. Mannitol
- C. Mechanical thrombectomy (Correct Answer)
- D. IV tPA
- E. Low molecular weight heparin
Stroke Explanation: ***Mechanical thrombectomy***
- The patient presents with **acute ischemic stroke** symptoms (aphasia, right-sided weakness, sensory deficits) at **5 hours from symptom onset**. Imaging (CTA showing large vessel occlusion and MRI confirming diffusion restriction) demonstrates a **large vessel occlusion**, making him a candidate for **mechanical thrombectomy**.
- Since the patient is **beyond the 4.5-hour window for IV tPA**, mechanical thrombectomy is the **primary reperfusion therapy** indicated for large vessel occlusion strokes up to **24 hours** (with appropriate imaging showing salvageable tissue).
- Mechanical thrombectomy offers the best chance for complete recanalization and improved neurological outcomes in large vessel occlusion strokes, particularly when IV tPA is not an option.
*Aspirin*
- While **aspirin** is crucial for **secondary stroke prevention**, it is not the primary acute treatment for a large vessel occlusion stroke due to its limited ability to achieve rapid and complete recanalization.
- Aspirin (or other antiplatelet therapy) is typically initiated **within 24-48 hours after stroke onset**, but only after excluding hemorrhagic transformation and after acute reperfusion therapies have been considered or completed.
*Mannitol*
- **Mannitol** is an osmotic diuretic used to reduce **intracranial pressure (ICP)** in cases of severe cerebral edema, which can be a complication of large ischemic strokes.
- It is not a primary treatment for the acute ischemic event itself, but rather a supportive measure used to manage life-threatening complications if **cerebral edema** develops and causes significant mass effect or herniation risk.
*IV tPA*
- **Intravenous tissue plasminogen activator (IV tPA)** is the first-line pharmacologic treatment for acute ischemic stroke if administered **within 4.5 hours of symptom onset** in eligible patients.
- This patient presents at **5 hours**, which is **beyond the approved time window** for IV tPA administration, making him **ineligible** for thrombolytic therapy.
- Even if within the time window, patients with large vessel occlusion often require mechanical thrombectomy in addition to or instead of IV tPA for optimal outcomes.
*Low molecular weight heparin*
- **Low molecular weight heparin (LMWH)** is primarily used for **deep vein thrombosis (DVT)** prophylaxis in immobilized patients or for the treatment of established DVT/pulmonary embolism.
- It is generally **not recommended for acute ischemic stroke treatment** due to an increased risk of hemorrhagic transformation without proven benefit in recanalization or clinical outcomes.
Stroke US Medical PG Question 2: A 78-year-old woman is accompanied by her family for a routine visit to her primary care provider. The family states that 5 months prior, the patient had a stroke and is currently undergoing physical therapy. Today, her temperature is 98.2°F (36.8°C), blood pressure is 112/72 mmHg, pulse is 64/min, and respirations are 12/min. On exam, she is alert and oriented with no deficits in speech. Additionally, her strength and sensation are symmetric and preserved bilaterally. However, on further neurologic testing, she appears to have some difficulty with balance and a propensity to fall to her right side. Which of the following deficits does the patient also likely have?
- A. Hemiballismus
- B. Hemispatial neglect
- C. Intention tremor
- D. Contralateral eye deviation
- E. Truncal ataxia (Correct Answer)
Stroke Explanation: ***Truncal ataxia***
- This patient's symptoms of **difficulty with balance** and a **propensity to fall to her right side** are highly suggestive of truncal ataxia.
- While she had a stroke, her preserved speech, symmetric strength and sensation, and alertness rule out typical hemiparesis or aphasia, pointing towards a **cerebellar lesion** affecting balance and coordination.
*Hemiballismus*
- This condition involves **flailing, high-amplitude, involuntary movements** typically affecting one side of the body.
- The patient's description of balance issues and falling, without mention of such specific movements, makes hemiballismus less likely.
*Hemispatial neglect*
- Characterized by the **inability to attend to one side of the environment**, usually the left side following a right parietal stroke.
- The patient's presentation does not describe an indifference to one side of her visual or personal space.
*Intention tremor*
- An **intention tremor** is a tremor that worsens during purposeful movement towards a target.
- While it can be associated with cerebellar dysfunction, the primary deficit described is imbalance and falling to one side, not specifically a tremor.
*Contralateral eye deviation*
- This typically occurs in acute stroke scenarios as part of a **gaze preference**, where the eyes deviate towards the side of the lesion (or away from the hemiparesis).
- The patient is 5 months post-stroke and is alert with no acute focal deficits, making acute eye deviation unlikely as a chronic presenting symptom here.
Stroke US Medical PG Question 3: A 67-year-old man with a past medical history of poorly-controlled type 2 diabetes mellitus (T2DM) is brought to the emergency department for acute onset nausea and vomiting. According to the patient, he suddenly experienced vertigo and began vomiting 3 hours ago while watching TV. He reports hiking in New Hampshire with his wife 2 days ago. Past medical history is significant for a myocardial infarction (MI) that was treated with cardiac stenting, T2DM, and hypertension. Medications include lisinopril, aspirin, atorvastatin, warfarin, and insulin. Physical examination demonstrates left-sided facial droop and decreased pinprick sensation at the right arm and leg. What is the most likely etiology of this patient’s symptoms?
- A. Hypoperfusion of the anterior spinal artery (ASA)
- B. Labyrinthitis
- C. Early disseminated Lyme disease
- D. Thrombotic stroke at the anterior inferior cerebellar artery (AICA)
- E. Embolic stroke at the posterior inferior cerebellar artery (PICA) (Correct Answer)
Stroke Explanation: ***Embolic stroke at the posterior inferior cerebellar artery (PICA)***
- The constellation of left-sided **facial droop** (cranial nerve impairment) and **contralateral decreased pinprick sensation** (spinothalamic tract deficit) in the context of acute vertigo, nausea, and vomiting is classic for a **lateral medullary syndrome (Wallenberg syndrome)**.
- Wallenberg syndrome is most commonly caused by an **ischemic stroke in the PICA territory**, often embolic, especially in patients with risk factors like **atrial fibrillation** (implied by warfarin use) or a history of MI.
*Hypoperfusion of the anterior spinal artery (ASA)*
- **ASA syndrome** typically presents with sudden onset **flaccid paraplegia, loss of pain and temperature sensation below the level of the lesion**, and preservation of proprioception and vibration sense.
- It does not typically cause **facial droop** or **vertigo**, as these are signs of brainstem involvement.
*Labyrinthitis*
- **Labyrinthitis** is an inflammation of the inner ear, causing acute onset **vertigo, nausea, vomiting**, and sometimes hearing loss or tinnitus.
- It would **not cause neurological deficits** like facial droop or contralateral sensory loss in the extremities, which are indicative of a central neurological event.
*Early disseminated Lyme disease*
- **Early disseminated Lyme disease** can cause neurological symptoms, including **facial nerve palsy** (often bilateral), but it typically presents with other symptoms like **meningitis, radiculopathy, or carditis**.
- The **hyperacute onset (3 hours)** strongly favors an acute vascular event over Lyme disease, which takes **days to weeks** to develop neurological manifestations after tick exposure.
*Thrombotic stroke at the anterior inferior cerebellar artery (AICA)*
- An **AICA stroke** typically presents with **ipsilateral facial paralysis, ipsilateral hearing loss**, vertigo, nystagmus, and sometimes contralateral loss of pain and temperature sensation.
- While it can cause vertigo and facial weakness, the specific pattern of **contralateral body sensory loss** combined with facial droop strongly points to a PICA distribution affecting the lateral medulla, not AICA.
Stroke US Medical PG Question 4: A 57-year-old man presents to the emergency department for evaluation of slurred speech and left arm and leg weakness over the last 3 hours. History reveals hypertension that is being treated with hydrochlorothiazide. Vital signs include: blood pressure of 110/70 mm Hg, heart rate 104/min, respiratory rate 18/min, and temperature 36.6°C (98.0°F). Physical examination reveals 2/5 strength in both left upper and lower extremities. After 2 hours, the patient’s symptoms suddenly disappear. An electrocardiogram (ECG) is obtained (see image). Which of the following medications could prevent ischemic attacks in this patient in the future?
- A. Warfarin (Correct Answer)
- B. Acetylsalicylic acid
- C. Enoxaparin
- D. Heparin
- E. Clopidogrel
Stroke Explanation: ***Warfarin***
- The patient experienced a **transient ischemic attack (TIA)** due to the sudden onset of neurological symptoms that resolved completely. The ECG shows **atrial fibrillation (AFib)**, characterized by an irregularly irregular rhythm and absence of P waves, which is a significant risk factor for cardioembolic stroke.
- **Oral anticoagulation** is essential for preventing ischemic stroke in patients with AFib. While **direct oral anticoagulants (DOACs)** such as apixaban, rivaroxaban, or dabigatran are now preferred as first-line therapy per current guidelines, **warfarin** remains an effective alternative and is the only oral anticoagulant option listed here.
- Warfarin prevents the formation of blood clots in the heart chambers by inhibiting vitamin K-dependent clotting factors, thereby reducing the risk of cardioembolic stroke.
*Acetylsalicylic acid*
- **Aspirin (acetylsalicylic acid)** is an antiplatelet agent used for primary and secondary prevention of ischemic stroke, particularly in patients with non-cardioembolic causes.
- While aspirin can be used in some cases, its efficacy in preventing stroke in patients with AFib is **significantly lower than that of oral anticoagulants** like warfarin or DOACs (reduces stroke risk by ~20% vs ~60-70% with anticoagulation).
*Enoxaparin*
- **Enoxaparin** is a low molecular weight heparin, an anticoagulant typically used for the **acute treatment** of deep vein thrombosis (DVT) and pulmonary embolism (PE), and sometimes as a bridge to warfarin therapy.
- It is not routinely used for **long-term prevention** of ischemic stroke in patients with AFib due to its parenteral (subcutaneous) administration and the need for daily injections.
*Heparin*
- **Heparin** (unfractionated) is an anticoagulant used for acute management of thrombotic events but requires continuous intravenous infusion and close monitoring of aPTT.
- Similar to enoxaparin, it is not practical or recommended for **long-term outpatient prophylaxis** against stroke in AFib.
*Clopidogrel*
- **Clopidogrel** is an antiplatelet agent that inhibits platelet aggregation via P2Y12 receptor blockade and is used in patients with atherosclerotic disease or as an alternative to aspirin in certain circumstances.
- It works by a different mechanism than anticoagulants and is generally **less effective than warfarin or DOACs** for preventing cardioembolic stroke from AFib (similar efficacy to aspirin alone).
Stroke US Medical PG Question 5: A 62-year-old man is brought to the emergency department by his wife because she thinks he has had a stroke. He has hypertension and type 2 diabetes mellitus. Current medications include enalapril and metformin. He has smoked 1 pack of cigarettes per day for the past 35 years. His blood pressure is 162/95 mm Hg. A CT scan of the brain shows a lacunar stroke involving the left subthalamic nucleus. The patient most likely presented with which of the following findings on physical examination?
- A. Cogwheel rigidity
- B. Dystonia
- C. Hemispatial agnosia
- D. Vertical gaze palsy
- E. Hemiballismus (Correct Answer)
Stroke Explanation: ***Hemiballismus***
- A lacunar stroke in the **subthalamic nucleus (STN)** typically causes **hemiballismus**, which is characterized by wild, involuntary, large-amplitude flinging movements on one side of the body.
- The STN is part of the **basal ganglia circuit** and its damage leads to disinhibition of the thalamus, resulting in hyperkinetic movements.
*Cogwheel rigidity*
- This is a feature of **Parkinson's disease**, resulting from damage to the **substantia nigra** affecting dopamine production, not typically a direct result of a lacunar stroke in the subthalamic nucleus.
- It is characterized by a jerky resistance to passive movement in a limb.
*Dystonia*
- Characterized by sustained or repetitive muscle contractions resulting in **twisting and repetitive movements** or abnormal fixed postures.
- While basal ganglia dysfunction can cause dystonia, it's a broader term, and **hemiballismus** is a more specific and classic presentation of STN lesions.
*Hemispatial agnosia*
- Refers to a deficit in attention to one side of space, most commonly associated with lesions in the **non-dominant (right) parietal lobe**.
- This is distinct from the motor symptoms expected from a subthalamic nucleus lesion.
*Vertical gaze palsy*
- Commonly associated with lesions in the **midbrain**, particularly the **dorsal midbrain syndrome (Parinaud syndrome)**.
- This is not a typical presentation of a lacunar stroke specifically involving the subthalamic nucleus.
More Stroke US Medical PG questions available in the OnCourse app. Practice MCQs, flashcards, and get detailed explanations.