IBD US Medical PG Practice Questions and MCQs
Practice US Medical PG questions for IBD. These multiple choice questions (MCQs) cover important concepts and help you prepare for your exams.
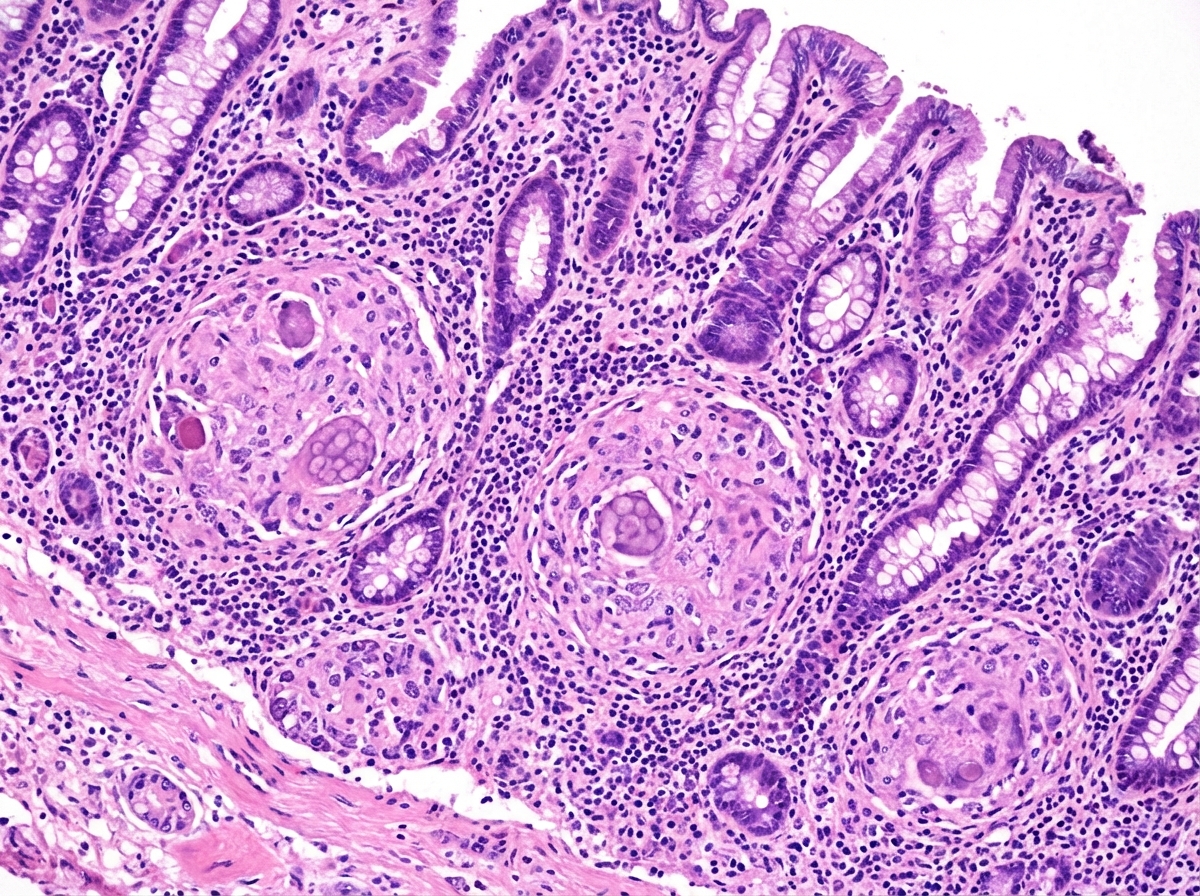
IBD US Medical PG Question 1: A 63-year-old man comes to the physician with a 4-week history of fatigue, crampy abdominal pain, watery diarrhea, and pain in his mouth and gums. He returned from a 2-week trip to the Dominican Republic 2 months ago. He has smoked one pack of cigarettes daily for 45 years. Examination shows three 1.5-cm, painful ulcers in the mouth. Abdominal examination shows mild tenderness to palpation in the right lower quadrant without guarding or rebound. His hemoglobin concentration is 11.2 g/dL, mean corpuscular volume is 75 fL, and leukocyte count is 11,900/mm³. Colonoscopy shows a cobblestone mucosa. A photomicrograph of a biopsy specimen is shown. Which of the following is the most likely diagnosis?
- A. Behcet disease
- B. Tropical sprue
- C. Ulcerative colitis
- D. Crohn disease (Correct Answer)
- E. Whipple disease
IBD Explanation: ***Crohn disease***
- The combination of **crampy abdominal pain**, **watery diarrhea**, **oral ulcers**, and **cobblestone mucosa** seen on colonoscopy strongly suggests Crohn disease. Crohn disease can affect any part of the gastrointestinal tract from mouth to anus, and oral manifestations like aphthous ulcers are common.
- The **microcytic anemia** (hemoglobin 11.2 g/dL, MCV 75 fL) is consistent with **chronic blood loss** and **iron malabsorption** often seen in Crohn disease. The elevated leukocyte count (11,900/mm³) indicates inflammation.
*Behcet disease*
- Behcet disease is characterized by recurrent **oral aphthous ulcers**, genital ulcers, and uveitis. While oral ulcers are present, the significant **gastrointestinal symptoms** (crampy abdominal pain, watery diarrhea, cobblestone mucosa) are not typical primary features of Behcet disease.
- Although it can rarely involve the GI tract, it typically doesn't present with extensive bowel involvement resembling inflammatory bowel disease to this degree, nor does it typically cause microcytic anemia from chronic GI blood loss.
*Tropical sprue*
- Tropical sprue typically presents with chronic **malabsorption**, foul-smelling diarrhea, and weight loss, occurring after travel to tropical regions. While the patient visited the Dominican Republic, the key findings of **oral ulcers** and **cobblestone mucosa** are not characteristic of tropical sprue.
- Tropical sprue is primarily a disease of the small intestine characterized by villous atrophy, not typically presenting with the "cobblestone" appearance associated with transmural inflammation seen in Crohn’s.
*Ulcerative colitis*
- Ulcerative colitis is characterized by continuous inflammation of the **colon and rectum**, typically presenting with bloody diarrhea and abdominal pain. While GI symptoms are present, the patient's **oral ulcers** and the finding of **cobblestone mucosa** strongly argue against ulcerative colitis.
- Ulcerative colitis affects only the colon and does not cause oral ulcers or skip lesions or transmural inflammation; the "cobblestone" appearance is indicative of deep fissures and ulcers separated by edematous mucosa, characteristic of Crohn disease.
*Whipple disease*
- Whipple disease is a rare systemic infection caused by *Tropheryma whipplei*, presenting with malabsorption, arthralgia, neurological symptoms, and lymphadenopathy. While GI symptoms like diarrhea and abdominal pain may occur, **oral ulcers** are not a typical feature, and the **colonoscopy findings** (cobblestone mucosa) are not characteristic of Whipple disease.
- Biopsy in Whipple disease would show **foamy macrophages** in the lamina propria that stain positive with periodic acid-Schiff (PAS), which is not indicated by the provided information.
IBD US Medical PG Question 2: A 33-year-old woman with Crohn’s disease colitis presents to her physician after 2 days of photophobia and blurred vision. She has had no similar episodes in the past. She has no abdominal pain or diarrhea and takes mesalazine, azathioprine, and prednisone as maintenance therapy. Her vital signs are within normal range. Examination of the eyes shows conjunctival injection. The physical examination is otherwise normal. Slit-lamp examination by an ophthalmologist shows evidence of inflammation in the anterior chamber. Which of the following is the most appropriate modification to this patient’s medication at this time?
- A. Adding infliximab
- B. Increasing dose of prednisone (Correct Answer)
- C. No modification of therapy at this time
- D. Discontinuing mesalazine
- E. Decreasing dose of azathioprine
IBD Explanation: ***Increasing dose of prednisone***
- This patient is presenting with **anterior uveitis**, a common **extraintestinal manifestation of Crohn’s disease**, characterized by photophobia, blurred vision, and inflammation of the anterior chamber.
- **Corticosteroids** (like prednisone) are the **first-line treatment for acute uveitis**, and increasing the dose will help control the inflammation effectively.
*Adding infliximab*
- While **biologics like infliximab** can be effective for refractory uveitis or systemic disease control, they are **not the immediate first-line treatment for an acute uveitis flare**, especially when corticosteroids are already part of the regimen.
- Adding a new biologic would also involve a longer onset of action and additional risks, making it less suitable for urgent symptom control compared to adjusting prednisone.
*No modification of therapy at this time*
- The patient clearly has **acute anterior uveitis**, which is a potentially serious ocular condition requiring prompt treatment to prevent complications such as synechiae, glaucoma, and vision loss.
- Doing nothing would lead to worsening inflammation and potential irreversible damage.
*Discontinuing mesalazine*
- **Mesalazine** (an aminosalicylate) is primarily used for maintaining remission in inflammatory bowel disease and is **not implicated in causing uveitis**, nor is discontinuing it a treatment for uveitis.
- It would also risk a flare of her Crohn's disease.
*Decreasing dose of azathioprine*
- **Azathioprine** is an **immunosuppressant** used to maintain remission in Crohn’s disease and is not a direct treatment for acute uveitis.
- Decreasing the dose would weaken her overall immunosuppression, potentially leading to a flare of her Crohn's disease or making her more susceptible to other issues, without directly addressing the acute ocular inflammation.
IBD US Medical PG Question 3: An 18-year-old man presents with bloody diarrhea and weight loss. He undergoes endoscopic biopsy which shows pseudopolyps. Biopsies taken during the endoscopy show inflammation only involving the mucosa and submucosa. He is diagnosed with an inflammatory bowel disease. Which of the following characteristics was most likely present?
- A. Cobblestone mucosa
- B. Skip lesions
- C. Fistulas and strictures
- D. Noncaseating granuloma
- E. Rectal involvement (Correct Answer)
IBD Explanation: **_Rectal involvement_**
- The description of **bloody diarrhea** and **pseudopolyps** on endoscopy, along with inflammation limited to the **mucosa and submucosa**, is highly characteristic of **ulcerative colitis (UC)**. UC invariably involves the rectum and extends proximally in a continuous fashion.
- The presence of **pseudopolyps** is common in UC due to cycles of mucosal ulceration and regeneration.
*Cobblestone mucosa*
- **Cobblestone mucosa** is a classic endoscopic finding in **Crohn's disease**, resulting from deep ulcerations interspersed with islands of edematous, non-ulcerated mucosa.
- This feature points to a transmural pattern of inflammation, which is inconsistent with the superficial inflammation confined to the **mucosa and submucosa** described.
*Skip lesions*
- **Skip lesions** refer to discontinuous areas of inflammation separated by healthy tissue, a hallmark feature of **Crohn's disease**.
- **Ulcerative colitis** (implied by the superficial inflammation) is characterized by continuous inflammation extending proximally from the rectum without skipped areas.
*Fistulas and strictures*
- **Fistulas** (abnormal connections between organs or to the skin) and **strictures** (narrowing of the intestinal lumen) are complications typically associated with **Crohn's disease**, due to its **transmural inflammation**.
- These are rare in **ulcerative colitis**, which primarily affects the superficial layers of the colon.
*Noncaseating granuloma*
- The presence of **noncaseating granulomas** on biopsy is a key histological feature distinguishing **Crohn's disease** from ulcerative colitis.
- The inflammation described as restricted to the **mucosa and submucosa** makes granulomas less likely, as they often imply a transmural process.
IBD US Medical PG Question 4: A 33-year-old man has a history of intermittent bloody diarrhea, tenesmus, fever, fatigue, and lower abdominal cramps for the past 2 weeks. On physical examination, he is lethargic and appears lean and pale. He has aphthous stomatitis, red congested conjunctiva, and tender swollen joints. At the doctor’s office, his pulse is 114/min, blood pressure is 102/76 mm Hg, respirations are 20/min, and his temperature is 39.4°C (102.9°F). There is vague lower abdominal tenderness and frank blood on rectal examination. Laboratory studies show:
Hemoglobin 7.6 g/dL
Hematocrit 33%
Total leucocyte count 22,000/mm3
Stool assay for C.difficile is negative
Abdominal X-ray shows no significant abnormality
He is symptomatically managed and referred to a gastroenterologist, who suggests a colonoscopy and contrast (barium) study for the diagnosis. Which of the following is the most likely combination of findings in his colonoscopy and barium study?
- A. Colonoscopy: Multiple vascular malformations that resemble telangiectasias on the colon wall, Barium study: Normal
- B. Colonoscopy: Patches of mucosal erosions with pseudomembrane formation, Barium study: Cobblestone appearance with strictures
- C. Colonoscopy: Discontinuous transmural ‘skip lesions’ with aphthoid linear ulcers and transverse fissures, non-caseating granulomas, and strictures, Barium study: Cobblestone appearance with strictures
- D. Colonoscopy: Normal, Barium study: Lead pipe colon appearance
- E. Colonoscopy: Continuous ulcerated lesions involving the mucosa and submucosa, granular mucosa, crypt abscess, and pseudopolyps, Barium study: Lead pipe colon appearance (Correct Answer)
IBD Explanation: ***Colonoscopy: Continuous ulcerated lesions involving the mucosa and submucosa granular mucosa, crypt abscess, and pseudopolyps, Barium study: Lead pipe colon appearance***
- The patient's symptoms (bloody diarrhea, tenesmus, fever, fatigue, weight loss, aphthous stomatitis, red congested conjunctiva, tender swollen joints, anemia, high WBC count) are highly suggestive of **Ulcerative Colitis (UC)**.
- **UC** on colonoscopy is characterized by **continuous mucosal and submucosal inflammation**, granular mucosa, crypt abscesses, and **pseudopolyps**. The barium study finding of a **"lead pipe" colon** is classic for long-standing UC due to loss of haustrations.
*Colonoscopy: Multiple vascular malformations that resemble telangiectasias on the colon wall, Barium study: Normal*
- **Angiodysplasia** presents with vascular malformations, but it typically causes painless lower GI bleeding, not the inflammatory symptoms described.
- The patient's severe systemic symptoms (fever, weight loss, anemia, high WBC) are inconsistent with angiodysplasia.
*Colonoscopy: Patches of mucosal erosions with pseudomembrane formation, Barium study: Cobblestone appearance with strictures*
- **Pseudomembrane formation** is characteristic of **_Clostridioides difficile_ infection**, which has been ruled out by the stool assay.
- While "cobblestone appearance" and strictures can be seen in inflammatory bowel disease, the pseudomembranes point away from UC or Crohn's.
*Colonoscopy: Discontinuous transmural ‘skip lesions’ with aphthoid linear ulcers and transverse fissures, non-caseating granulomas, and strictures, Barium study: Cobblestone appearance with strictures*
- This description is characteristic of **Crohn's disease**, which involves **discontinuous**, **transmural inflammation** with **skip lesions**, aphthoid ulcers, and non-caseating granulomas.
- While some symptoms overlap with UC, the involvement of mucocutaneous lesions and generalized systemic symptoms fits better with the continuous inflammation of UC than the patchy disease of Crohn's.
*Colonoscopy: Normal, Barium study: Lead pipe colon appearance*
- A **normal colonoscopy** would be inconsistent with the patient's severe symptoms of bloody diarrhea, anemia, and elevated inflammatory markers.
- A "lead pipe" colon indicates chronic inflammatory changes, which would undoubtedly be visible on colonoscopy.
IBD US Medical PG Question 5: A 31-year-old man presents to an urgent care clinic with symptoms of lower abdominal pain, bloating, bloody diarrhea, and fullness, all of which have become more frequent over the last 3 months. His vital signs are as follows: blood pressure is 121/81 mm Hg, heart rate is 87/min, and respiratory rate is 15/min. Rectal examination reveals a small amount of bright red blood. Lower endoscopy is performed, showing extensive mucosal erythema, induration, and pseudopolyps extending from the rectum to the splenic flexure. Given the following options, what is the most appropriate initial treatment for this patient's underlying disease?
- A. Azathioprine
- B. Mesalamine (Correct Answer)
- C. Systemic corticosteroids
- D. Total proctocolectomy
- E. Sulfasalazine
IBD Explanation: ***Mesalamine***
- The patient's symptoms (bloody diarrhea, abdominal pain, erythema, pseudopolyps, and inflammation extending from the rectum to the splenic flexure) are highly suggestive of **ulcerative colitis (UC) affecting the left colon (distal colitis)**.
- **Mesalamine** (a 5-aminosalicylic acid or 5-ASA derivative) is the first-line treatment for mild to moderate UC, especially for proctitis and left-sided colitis. Its anti-inflammatory action is exerted topically on the colonic mucosa.
*Azathioprine*
- Azathioprine is an **immunomodulator** used for maintaining remission in UC or in cases where patients are steroid-dependent or refractory to 5-ASAs.
- It is not typically used as a first-line agent for acute, mild to moderate disease.
*Systemic corticosteroids*
- **Systemic corticosteroids** are used for moderate to severe UC or for severe flares, not for initial mild to moderate disease, due to their significant side effect profile.
- While effective in inducing remission, their long-term use is limited, and they are not considered a maintenance therapy.
*Total proctocolectomy*
- **Total proctocolectomy** is a surgical option reserved for severe, refractory UC that does not respond to medical therapy, or in cases of dysplasia/cancer.
- It is an invasive procedure and not an appropriate initial treatment for a patient presenting with symptoms of mild to moderate disease.
*Sulfasalazine*
- **Sulfasalazine** is an older 5-ASA compound that is also effective for mild to moderate UC.
- However, it has a **higher incidence of side effects** (e.g., GI upset, headaches, hypersensitivity) compared to mesalamine, making mesalamine generally preferred for better tolerability.
More IBD US Medical PG questions available in the OnCourse app. Practice MCQs, flashcards, and get detailed explanations.