Hematology (anemias, clotting disorders) US Medical PG Practice Questions and MCQs
Practice US Medical PG questions for Hematology (anemias, clotting disorders). These multiple choice questions (MCQs) cover important concepts and help you prepare for your exams.
Hematology (anemias, clotting disorders) US Medical PG Question 1: A 25-year-old African-American woman visits the doctor’s office complaining of fatigue for a couple of months. She says that she feels exhausted by the end of the day. She works as a dental assistant and is on her feet most of the time. However, she eats well and also tries to walk for 30 minutes every morning. She also says that she sometimes feels breathless and has to gasp for air, especially when she is walking or jogging. Her past medical history is insignificant, except for occasional bouts of cold during the winters. Her physical exam findings are within normal limits except for moderate conjunctival pallor. Complete blood count results and iron profile are as follows:
Hemoglobin 9 g/dL
Hematocrit 28.5%
RBC count 5.85 x 106/mm3
WBC count 5,500/mm3
Platelet count 212,000/mm3
MCV 56.1 fl
MCH 20.9 pg/cell
MCHC 25.6 g/dL
RDW 11.7% Hb/cell
Serum iron 170 mcg/dL
Total iron-binding capacity (TIBC) 458 mcg/dL
Transferrin saturation 60%
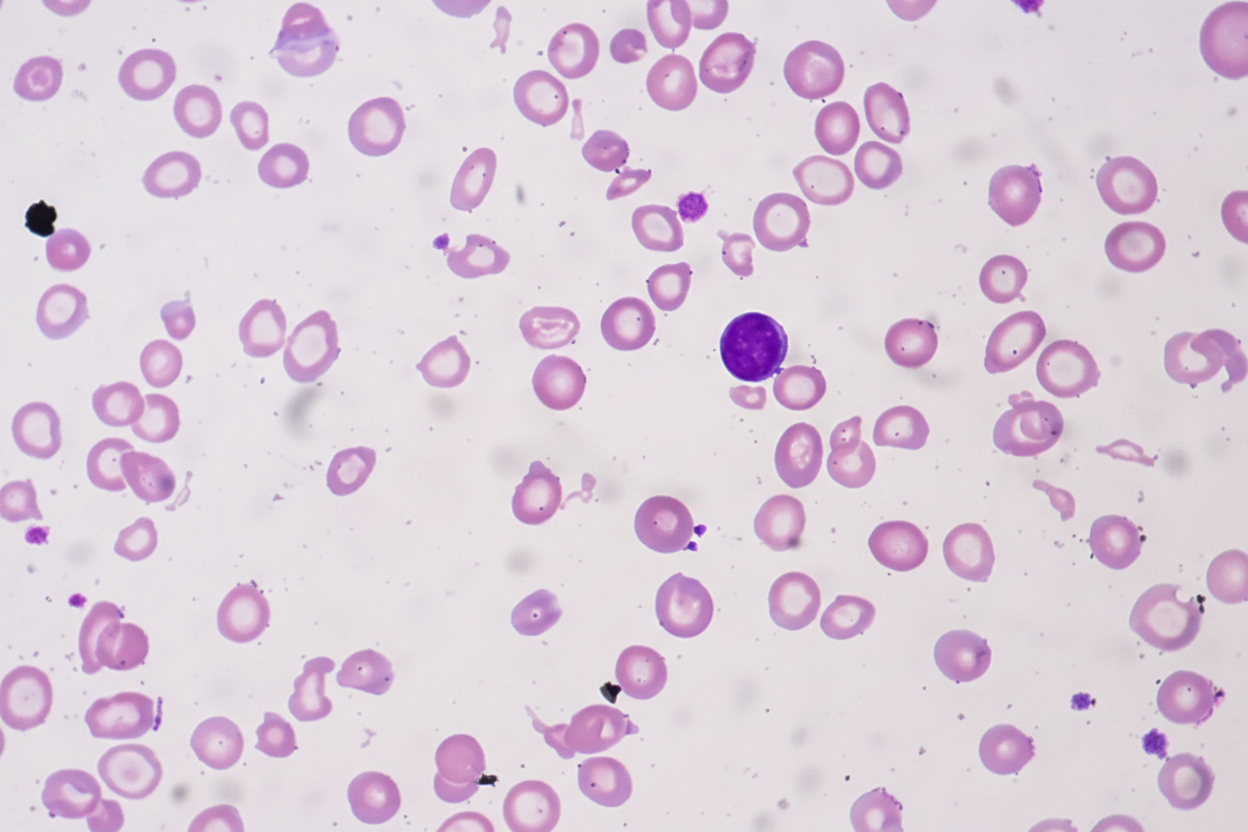
A peripheral blood smear is given. When questioned about her family history of anemia, she says that all she remembers is her dad was never allowed to donate blood as he was anemic. Which of the following most likely explains her cell counts and blood smear results?
- A. Thalassemia (Correct Answer)
- B. Iron-deficiency anemia
- C. B12 deficiency
- D. Hemolysis
- E. Folate deficiency
Hematology (anemias, clotting disorders) Explanation: ***Thalassemia***
- The patient presents with **microcytic, hypochromic anemia** (low MCV, MCH, MCHC) despite elevated iron stores, which is characteristic of thalassemia.
- The **elevated RBC count** (5.85 x 10^6/mm³) in the presence of anemia (hemoglobin 9 g/dL) is a hallmark of thalassemia, as the body attempts to compensate for ineffective erythropoiesis.
- The **elevated serum iron (170 mcg/dL) and high transferrin saturation (60%)** indicate iron overload, not iron deficiency, which occurs in thalassemia due to ineffective erythropoiesis and increased iron absorption.
- The **low RDW (11.7%)** indicates uniform cell size despite microcytosis, typical of thalassemia (vs. high RDW in iron deficiency).
- **Positive family history** (father was anemic and couldn't donate blood) supports an inherited disorder.
*Iron-deficiency anemia*
- This condition typically presents with **low serum iron**, **high TIBC**, and **low transferrin saturation** (<20%), which contradicts the patient's iron profile showing elevated iron and high transferrin saturation (60%).
- While iron-deficiency anemia also causes **microcytic, hypochromic RBCs**, the RBC count would be low or normal (not elevated), and RDW would be elevated (>14%) due to anisocytosis.
*B12 deficiency*
- **B12 deficiency** causes **macrocytic anemia** (high MCV >100 fl), which is inconsistent with the patient's low MCV (56.1 fl).
- It also often presents with neurological symptoms (peripheral neuropathy, subacute combined degeneration), which are absent in this case.
*Hemolysis*
- While hemolysis can cause anemia and fatigue, it is usually associated with elevated **reticulocyte count**, **indirect bilirubin**, and **LDH**, and decreased **haptoglobin**, none of which are indicated here.
- Hemolysis typically presents with **normocytic anemia** (normal MCV), not the marked **microcytosis** (MCV 56.1 fl) seen in this patient.
*Folate deficiency*
- Similar to B12 deficiency, **folate deficiency** leads to **macrocytic anemia** (high MCV >100 fl), which is not observed in this patient with MCV of 56.1 fl.
- Folate deficiency does not cause neurological symptoms (unlike B12 deficiency), but the **macrocytic** red cell morphology is the key differentiator here.
Hematology (anemias, clotting disorders) US Medical PG Question 2: A 25-year-old woman is being evaluated due to complaint of fatigue and voiding pink urine. The laboratory results are as follows:
Hb 6.7
Red blood cell count 3.0 x 1012/L
Leukocyte count 5,000/mm3
Platelets 170 x 109/L
Reticulocyte count 6%
Hematocrit 32%
The physician thinks that the patient is suffering from an acquired mutation in hematopoietic stem cells, which is confirmed by flow cytometry analysis that revealed these cells are CD 55 and CD 59 negative. However, the physician is interested in knowing the corrected reticulocyte count before starting the patient on eculizumab. What value does the physician find after calculating the corrected reticulocyte count?
- A. 3.1%
- B. 0.4%
- C. 0.1%
- D. 0.6%
- E. 4.6% (Correct Answer)
Hematology (anemias, clotting disorders) Explanation: ***4.6%***
- The corrected reticulocyte count accounts for the degree of anemia by adjusting for the patient's hematocrit compared to normal.
- **Formula: Corrected Retics% = Observed Retics% × (Patient's Hct / Normal Hct)**
- Using normal Hct of 42% for women: 6% × (32/42) = 6% × 0.76 = **4.56% ≈ 4.6%**
- This reflects the actual reticulocyte production capacity adjusted for the anemic state.
*3.1%*
- This value might result from using an incorrect normal hematocrit value in the calculation.
- For example, using 6% × (32/60) would give approximately 3.2%, suggesting use of an inappropriately high reference value.
*0.4%*
- This value likely results from applying the **Reticulocyte Production Index (RPI)** formula, which includes a maturation factor correction: 6% × (32/42) × (1/2.5) = 1.82%, then with further error.
- Such a low value from formula misapplication does not represent the standard corrected reticulocyte count requested.
*0.1%*
- This extremely low value would indicate **severe calculation error** or bone marrow failure, which contradicts the observed 6% reticulocyte count.
- In PNH with hemolysis, reticulocyte production is typically increased, making this value implausible.
*0.6%*
- This incorrect value could result from mathematical errors in applying correction factors or using the wrong hematocrit values in the formula.
- The standard corrected reticulocyte formula would not yield this value with the given parameters.
Hematology (anemias, clotting disorders) US Medical PG Question 3: An otherwise healthy 42-year-old man undergoes routine investigations prior to blood donation. His complete blood count is shown:
Hemoglobin 9.3 g/dL
Mean corpuscular volume (MCV) 71 μm3
Mean corpuscular hemoglobin (MCH) 21 pg/cell
White blood cell count 8,200/mm3
Platelet count 317,000/mm3
Iron studies are shown:
Serum iron 210 μg/dL
Serum ferritin 310 ng/mL
Total iron binding capacity (TIBC) 290 μg/dL
Transferrin saturation 78%
He occasionally drinks alcohol and denies smoking or use of illicit drugs. There is a family history of anemia including his brother and maternal uncle. Examination shows conjunctival pallor, but is otherwise unremarkable. Which of the following is the most likely diagnosis?
- A. Hemochromatosis
- B. Anemia of chronic disease
- C. Acute myeloid leukemia
- D. Sideroblastic anemia (Correct Answer)
- E. Myelodysplastic syndrome
Hematology (anemias, clotting disorders) Explanation: ***Sideroblastic anemia***
- The patient presents with **microcytic anemia** (Hb 9.3 g/dL, MCV 71, MCH 21) and evidence of **iron overload** (serum iron 210, ferritin 310, transferrin saturation 78%). These findings, along with a **family history of anemia affecting males** (brother and maternal uncle), are classic for **hereditary sideroblastic anemia**, typically X-linked.
- **Sideroblastic anemia** is characterized by the bone marrow producing ring sideroblasts (erythroblasts with iron-laden mitochondria), leading to ineffective erythropoiesis and iron accumulation.
- The hereditary form presents in younger patients with isolated anemia and strong family history, distinguishing it from acquired forms.
*Hemochromatosis*
- While **hemochromatosis** also presents with iron overload (high serum iron, ferritin, and transferrin saturation), it typically does **not cause microcytic anemia** or any significant anemia.
- The primary defect in hemochromatosis is increased iron absorption leading to tissue iron deposition (liver, heart, pancreas), without the erythropoietic dysfunction seen in sideroblastic anemia.
*Anemia of chronic disease*
- **Anemia of chronic disease (ACD)** typically presents with normal or slightly reduced MCV and MCH, and is characterized by **low serum iron** and **low TIBC**, with normal or elevated ferritin.
- In this case, the patient has **elevated serum iron** and **high transferrin saturation (78%)**, making ACD unlikely.
*Acute myeloid leukemia*
- **Acute myeloid leukemia (AML)** involves the proliferation of immature myeloid cells and usually presents with pancytopenia or symptoms related to bone marrow failure (e.g., fatigue, bleeding, infections).
- The blood counts here show **isolated anemia with normal WBC and platelet counts**, and the iron studies are not typical for AML.
*Myelodysplastic syndrome*
- **Myelodysplastic syndromes (MDS)** are clonal disorders of hematopoietic stem cells, often presenting with cytopenias and dysplastic features in the bone marrow.
- While **acquired sideroblastic anemia** is a subtype of MDS (refractory anemia with ring sideroblasts), it typically occurs in **older adults (>60 years)** without a family history.
- This patient's **young age (42 years)** and **strong family history** (brother and maternal uncle) point to **hereditary sideroblastic anemia** rather than MDS-associated acquired sideroblastic anemia.
Hematology (anemias, clotting disorders) US Medical PG Question 4: A 10-year-old girl with previously diagnosed sickle cell anemia presents to the emergency room with a low-grade fever, malaise, petechiae on her arms, and a rash on her face. She regularly takes hydroxyurea and receives blood transfusions to treat her condition. Her blood tests show a hemoglobin of 4.0 g/dL, MCV of 87 fl, and 2% reticulocyte count. An attempted bone marrow biopsy was a dry, empty tap. What is the most likely diagnosis?
- A. Reaction to the blood transfusions
- B. Gastrointestinal bleeding
- C. Anemia of chronic disease
- D. Aplastic crisis (Correct Answer)
- E. Sequestration crisis
Hematology (anemias, clotting disorders) Explanation: ***Aplastic crisis***
- The combination of **severe anemia** (hemoglobin 4.0 g/dL), **low reticulocyte count** (2%), and a **dry bone marrow tap** confirms a defect in red blood cell production.
- In a patient with **sickle cell anemia**, an aplastic crisis is often triggered by **Parvovirus B19 infection**, which targets erythroid precursors.
*Reaction to the blood transfusions*
- An acute transfusion reaction would typically present with fever, chills, urticaria, or dyspnea, which are not the predominant symptoms here.
- Hemoglobin would likely drop acutely or remain stable, but not necessarily with such a profound reticulocytopenia or bone marrow findings.
*Gastrointestinal bleeding*
- While GI bleeding can cause severe anemia, it would typically be associated with **microcytic anemia** (decreased MCV if chronic) and **elevated reticulocyte count** as the bone marrow tries to compensate, neither of which are observed.
- There is no mention of melena or hematochezia, and the dry bone marrow tap points to a production problem, not blood loss.
*Anemia of chronic disease*
- This condition typically results in **mild to moderate anemia** with a **normal or slightly reduced MCV** and a **low reticulocyte count**.
- However, the hemoglobin level of 4.0 g/dL is too severe for typical anemia of chronic disease, and the dry bone marrow tap is not a characteristic finding.
*Sequestration crisis*
- A sequestration crisis involves the rapid pooling of blood in the spleen or liver, leading to **acute severe anemia** and often **splenomegaly**.
- However, it would be characterized by a **high reticulocyte count** as the bone marrow attempts to compensate for the sudden blood loss, which is contrary to the findings in this case.
Hematology (anemias, clotting disorders) US Medical PG Question 5: A 39-year-old woman presents with progressive weakness, exercise intolerance, and occasional dizziness for the past 3 months. Past medical history is unremarkable. She reports an 18-pack-year smoking history and drinks alcohol rarely. Her vital signs include: temperature 36.6°C (97.8°F), blood pressure 139/82 mm Hg, pulse 98/min. Physical examination is unremarkable. Her laboratory results are significant for the following:
Hemoglobin 9.2 g/dL
Erythrocyte count 2.1 million/mm3
Mean corpuscular volume (MCV) 88 μm3
Mean corpuscular hemoglobin (MCH) 32 pg/cell
Leukocyte count 7,500/mm3
Which of the following is the best next step in the management of this patient’s condition?
- A. Serum ferritin level
- B. Direct antiglobulin test
- C. C-reactive protein (CRP)
- D. Bone marrow biopsy
- E. Reticulocyte count (Correct Answer)
Hematology (anemias, clotting disorders) Explanation: ***Reticulocyte count***
- A **normocytic anemia** (MCV 88) with signs of weakness and exercise intolerance requires evaluation of **red blood cell production**.
- A reticulocyte count helps differentiate between **hypoproliferative** (low count) and **hyperproliferative** (high count) anemias, guiding further diagnostic steps.
*Serum ferritin level*
- While often low in **iron-deficiency anemia**, this patient’s **normocytic MCV** makes iron deficiency less likely as the primary cause without other features.
- A normal ferritin doesn't rule out other causes of anemia, and a high ferritin could indicate **anemia of chronic disease**, but further understanding of RBC production is needed first.
*Direct antiglobulin test*
- This test is used to diagnose **autoimmune hemolytic anemia**, which typically presents with **jaundice**, **splenomegaly**, and elevated **lactate dehydrogenase (LDH)**, none of which are noted here.
- While anemia can result from hemolysis, the initial presentation doesn't strongly suggest an immune-mediated destruction process, and determining the bone marrow's response is more immediate.
*C-reactive protein (CRP)*
- CRP is a marker of **inflammation**, and elevated levels could suggest **anemia of chronic disease**.
- However, knowing the **reticulocyte count** will provide more direct information about bone marrow function, which is crucial for characterizing the anemia.
*Bone marrow biopsy*
- A bone marrow biopsy is an **invasive procedure** typically reserved for complex anemias where initial, less invasive tests have failed to provide a diagnosis or when conditions like **aplastic anemia** or **myelodysplastic syndromes** are strongly suspected.
- It is not the appropriate **first diagnostic step** in evaluating an undifferentiated normocytic anemia like this.
More Hematology (anemias, clotting disorders) US Medical PG questions available in the OnCourse app. Practice MCQs, flashcards, and get detailed explanations.