Vascular supply (Circle of Willis) US Medical PG Practice Questions and MCQs
Practice US Medical PG questions for Vascular supply (Circle of Willis). These multiple choice questions (MCQs) cover important concepts and help you prepare for your exams.
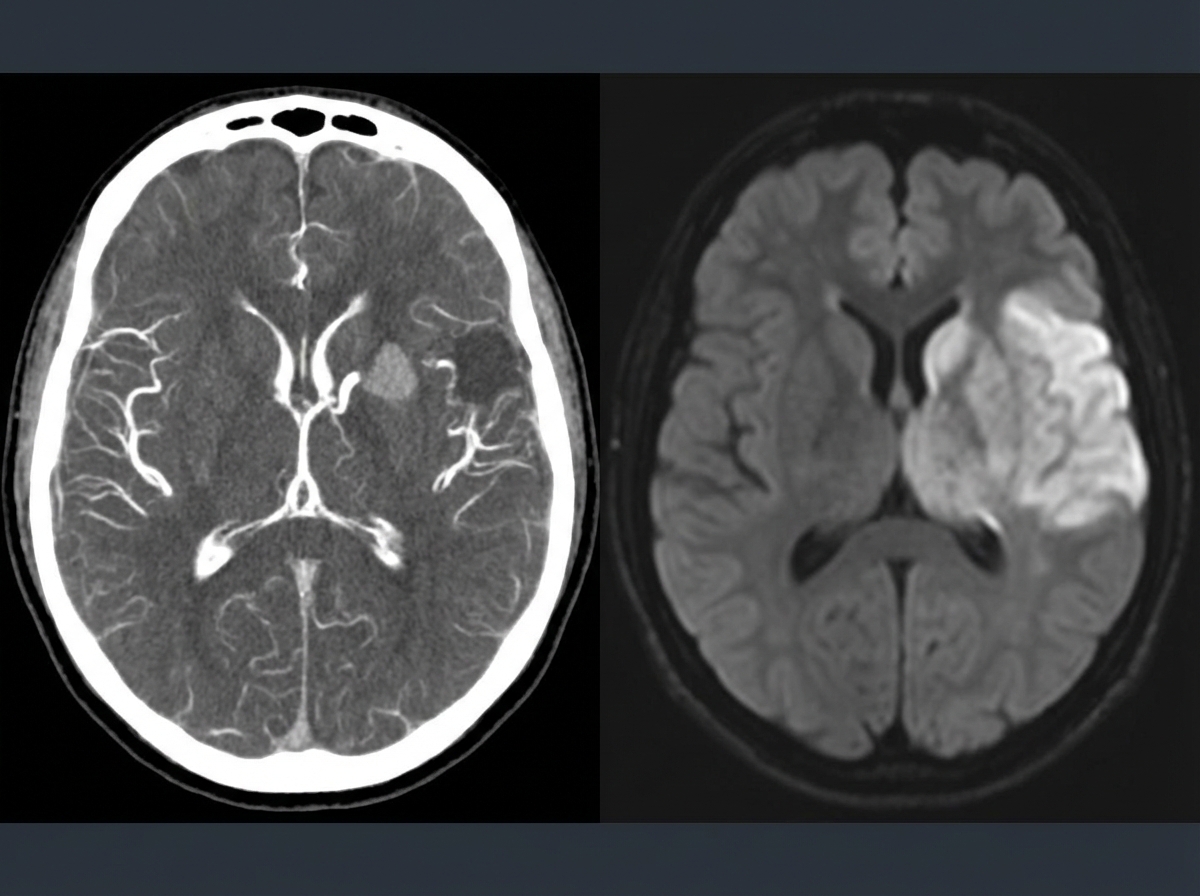
Vascular supply (Circle of Willis) US Medical PG Question 1: A 69-year-old man is brought in by his wife with acute onset aphasia for the past 5 hours. The patient's wife says that they were sitting having dinner when suddenly he was not able to speak. They delayed coming to the hospital because he had a similar episode 2 months ago which resolved within an hour. His past medical history is significant for hypercholesterolemia, managed with rosuvastatin, and a myocardial infarction (MI) 2 months ago, status post percutaneous transluminal coronary angioplasty complicated by residual angina. His family history is significant for his father who died of MI at age 60. The patient reports a 15-pack-year smoking history but denies any alcohol or recreational drug use. The vital signs include: temperature 37.0℃ (98.6℉), blood pressure 125/85 mm Hg, pulse 96/min, and respiratory rate 19/min. On physical examination, the patient has expressive aphasia. There is a weakness of the right-sided lower facial muscles. The strength in his upper and lower extremities is 4/5 on the right and 5/5 on the left. There is also a decreased sensation on his right side. A noncontrast computed tomography (CT) scan of the head is unremarkable. CT angiography (CTA) and diffusion-weighted magnetic resonance imaging (MRI) of the brain are acquired, and the findings are shown in the exhibit (see image). Which of the following is the best course of treatment in this patient?
- A. Aspirin
- B. Mannitol
- C. Mechanical thrombectomy (Correct Answer)
- D. IV tPA
- E. Low molecular weight heparin
Vascular supply (Circle of Willis) Explanation: ***Mechanical thrombectomy***
- The patient presents with **acute ischemic stroke** symptoms (aphasia, right-sided weakness, sensory deficits) at **5 hours from symptom onset**. Imaging (CTA showing large vessel occlusion and MRI confirming diffusion restriction) demonstrates a **large vessel occlusion**, making him a candidate for **mechanical thrombectomy**.
- Since the patient is **beyond the 4.5-hour window for IV tPA**, mechanical thrombectomy is the **primary reperfusion therapy** indicated for large vessel occlusion strokes up to **24 hours** (with appropriate imaging showing salvageable tissue).
- Mechanical thrombectomy offers the best chance for complete recanalization and improved neurological outcomes in large vessel occlusion strokes, particularly when IV tPA is not an option.
*Aspirin*
- While **aspirin** is crucial for **secondary stroke prevention**, it is not the primary acute treatment for a large vessel occlusion stroke due to its limited ability to achieve rapid and complete recanalization.
- Aspirin (or other antiplatelet therapy) is typically initiated **within 24-48 hours after stroke onset**, but only after excluding hemorrhagic transformation and after acute reperfusion therapies have been considered or completed.
*Mannitol*
- **Mannitol** is an osmotic diuretic used to reduce **intracranial pressure (ICP)** in cases of severe cerebral edema, which can be a complication of large ischemic strokes.
- It is not a primary treatment for the acute ischemic event itself, but rather a supportive measure used to manage life-threatening complications if **cerebral edema** develops and causes significant mass effect or herniation risk.
*IV tPA*
- **Intravenous tissue plasminogen activator (IV tPA)** is the first-line pharmacologic treatment for acute ischemic stroke if administered **within 4.5 hours of symptom onset** in eligible patients.
- This patient presents at **5 hours**, which is **beyond the approved time window** for IV tPA administration, making him **ineligible** for thrombolytic therapy.
- Even if within the time window, patients with large vessel occlusion often require mechanical thrombectomy in addition to or instead of IV tPA for optimal outcomes.
*Low molecular weight heparin*
- **Low molecular weight heparin (LMWH)** is primarily used for **deep vein thrombosis (DVT)** prophylaxis in immobilized patients or for the treatment of established DVT/pulmonary embolism.
- It is generally **not recommended for acute ischemic stroke treatment** due to an increased risk of hemorrhagic transformation without proven benefit in recanalization or clinical outcomes.
Vascular supply (Circle of Willis) US Medical PG Question 2: A 52-year-man is brought to the physician because of a 2-week history of memory loss. Three weeks ago, he had a cardiac arrest that required cardiopulmonary resuscitation and intravenous epinephrine. On mental status examination, he cannot recall objects shown to him 20 minutes earlier but vividly recalls memories from before the incident. The remainder of the examination shows no abnormalities. Which of the following structures of the brain is most likely affected?
- A. Internal pyramidal layer of the amygdala
- B. Microglial cells of dorsal midbrain
- C. Purkinje cells of the cerebellum
- D. Pyramidal cells of the hippocampus (Correct Answer)
- E. Astroglial cells of the putamen
Vascular supply (Circle of Willis) Explanation: ***Pyramidal cells of the hippocampus***
- The patient's inability to form new memories (anterograde amnesia) following a period of **hypoxia** suggests damage to the **hippocampus**, specifically its pyramidal cells.
- The **hippocampus** is highly vulnerable to **ischemic injury** due to the metabolic demands of its pyramidal cells.
*Internal pyramidal layer of the amygdala*
- The amygdala is primarily involved in **emotional processing**, particularly fear and anxiety, not memory encoding directly.
- Damage to the amygdala would likely manifest as altered emotional responses, rather than isolated memory loss.
*Microglial cells of dorsal midbrain*
- Microglial cells are the brain's resident immune cells and proliferate in response to injury, they are not the primary site of memory formation.
- The dorsal midbrain contains structures involved in visual and auditory reflexes, not directly memory consolidation.
*Purkinje cells of the cerebellum*
- Purkinje cells are specialized neurons in the **cerebellum** responsible for **motor coordination** and balance.
- Damage to these cells would result in ataxia and motor dysfunction, not memory deficits.
*Astroglial cells of the putamen*
- Astroglial cells are supportive cells throughout the brain; the putamen is involved in **motor control** and **procedural learning**.
- Dysfunction of the putamen typically leads to movement disorders like Parkinsonism, not specific memory loss.
Vascular supply (Circle of Willis) US Medical PG Question 3: A 59-year-old man is brought to the emergency department by his wife for a 1-hour history of sudden behavior changes. They were having lunch together when, at 1:07 PM, he suddenly dropped his sandwich on the floor. Since then, he has been unable to use his right arm. She also reports that he is slurring his speech and dragging his right foot when he walks. Nothing like this has ever happened before. The vital signs include: pulse 95/min, blood pressure 160/90 mm Hg, and respiratory rate 14/min. The physical exam is notable for an irregularly irregular rhythm on cardiac auscultation. On neurological exam, he has a facial droop on the right half of his face but is able to elevate his eyebrows symmetrically. He has 0/5 strength in his right arm, 2/5 strength in his right leg, and reports numbness throughout the right side of his body. Angiography of the brain will most likely show a lesion in which of the following vessels?
- A. Posterior cerebral artery
- B. Internal carotid artery
- C. Middle cerebral artery (Correct Answer)
- D. Basilar artery
- E. Anterior cerebral artery
Vascular supply (Circle of Willis) Explanation: ***Middle cerebral artery***
- The patient's symptoms, including **right-sided weakness with arm > leg involvement** (0/5 arm, 2/5 leg), **facial droop** (lower face sparing the forehead), and **slurred speech (dysarthria/aphasia)**, are classic signs of an **MCA stroke**.
- The **arm > leg pattern** is the key distinguishing feature of MCA territory infarction, as the MCA supplies the **lateral motor cortex** (which controls arm and face).
- The finding of an **irregularly irregular rhythm** suggests **atrial fibrillation**, a common cause of **embolic stroke** to the MCA.
*Posterior cerebral artery*
- PCA strokes primarily affect the **occipital lobe** and **medial temporal lobe**, leading to **visual field defects** (e.g., homonymous hemianopsia) or memory deficits.
- While it can cause sensory loss, it typically does not present with the **prominent motor deficits** and **facial droop** seen in this patient.
*Internal carotid artery*
- ICA occlusion can cause symptoms similar to MCA stroke, especially if the **MCA is a direct branch of the ICA**, or it can cause both MCA and ACA symptoms simultaneously.
- However, the specific constellation of symptoms described (predominant motor and sensory deficits, speech issues) points more directly to the **MCA territory downstream**.
*Basilar artery*
- Basilar artery strokes affect the **brainstem** and often present with a combination of **cranial nerve palsies**, **ataxia**, bilateral weakness, **vertigo**, and sometimes **"locked-in" syndrome**.
- The patient's symptoms are more consistent with a **hemispheric lesion**, not a brainstem lesion.
*Anterior cerebral artery*
- ACA strokes typically cause **contralateral leg > arm weakness** (opposite pattern from MCA), as the ACA supplies the **medial motor cortex**.
- ACA strokes may also present with **behavioral changes** (e.g., abulia, apathy) due to involvement of the frontal lobe.
- The patient's prominent **right arm weakness** and **facial droop** are not characteristic of an ACA stroke.
Vascular supply (Circle of Willis) US Medical PG Question 4: A 56-year-old man is brought to the emergency department 25 minutes after the sudden onset of severe pain in the middle of his chest. He describes the pain as tearing in quality; it radiates to his jaw. He has hypertension. He has smoked one pack of cigarettes daily for the 25 years. Current medications include enalapril. His blood pressure is 154/95 mm Hg in his right arm and 181/105 mm Hg in his left arm. A CT scan of the chest is shown. The structure indicated by the arrow is a derivative of which of the following?
- A. Right horn of sinus venosus
- B. Primitive atrium
- C. Right common cardinal vein
- D. Truncus arteriosus (Correct Answer)
- E. Bulbus cordis
Vascular supply (Circle of Willis) Explanation: ***Truncus arteriosus***
- This clinical scenario describes an **aortic dissection**, suggested by the sudden onset of **tearing chest pain radiating to the jaw**, significant **blood pressure differential** between arms, and presenting in a patient with **hypertension and smoking history**.
- The image likely shows a dilated aorta or an aortic dissection. The **truncus arteriosus** is the embryonic precursor to the **ascending aorta** and the **pulmonary trunk**, making it the correct derivative for the affected structure.
*Right horn of sinus venosus*
- The **right horn of the sinus venosus** primarily contributes to the formation of the **smooth-walled part of the right atrium** (sinus venarum).
- It does not give rise to the aorta, which is the structure involved in the described pathology.
*Primitive atrium*
- The **primitive atrium** develops into the **trabeculated parts** of both the **right and left atria** (atrial appendages).
- It is not involved in the formation of the great arteries like the aorta.
*Right common cardinal vein*
- The **right common cardinal vein** contributes to the formation of the **superior vena cava**.
- It is not a developmental source for the aorta.
*Bulbus cordis*
- The **bulbus cordis** gives rise to the **conus arteriosus** (infundibulum) of the right ventricle, the **aortic vestibule** of the left ventricle, and part of the **right ventricle**.
- While it is a component of the outflow tract, the primary structure from which the ascending aorta develops is the truncus arteriosus.
Vascular supply (Circle of Willis) US Medical PG Question 5: A researcher is studying the brains of patients who recently died from stroke-related causes. One specimen has a large thrombus in an area of the brain that is important in relaying many modalities of sensory information from the periphery to the sensory cortex. Which of the following embryologic structures gave rise to the part of the brain in question?
- A. Metencephalon
- B. Diencephalon (Correct Answer)
- C. Mesencephalon
- D. Telencephalon
- E. Myelencephalon
Vascular supply (Circle of Willis) Explanation: ***Diencephalon***
- The **thalamus**, a key relay center for sensory information to the cerebral cortex, develops from the diencephalon.
- A thrombus in this area would severely impair the transmission of **sensory modalities** from the periphery.
*Metencephalon*
- The metencephalon gives rise to the **pons** and the **cerebellum**.
- These structures are primarily involved in motor control, coordination, and respiratory regulation, not direct sensory relay to the cortex.
*Mesencephalon*
- The mesencephalon develops into the **midbrain**.
- The midbrain contains structures involved in visual and auditory reflexes, and motor control, but not the primary sensory relay described.
*Myelencephalon*
- The myelencephalon gives rise to the **medulla oblongata**.
- The medulla is crucial for vital autonomic functions (e.g., breathing, heart rate) and connects the brain to the spinal cord.
*Telencephalon*
- The telencephalon develops into the **cerebral hemispheres** (cerebral cortex, basal ganglia, hippocampus).
- While it processes sensory information, it is not the primary relay center from the periphery; that role belongs to the thalamus.
More Vascular supply (Circle of Willis) US Medical PG questions available in the OnCourse app. Practice MCQs, flashcards, and get detailed explanations.