
Imaging/Clinical
Complete Imaging/Clinical study resources for USMLE. Part of Anatomy.
Study Resources
Choose how you want to study Imaging/Clinical
Lessons
11 lessons in Imaging/Clinical

X-ray principles and interpretation

CT scan principles and interpretation

MRI principles and interpretation

Ultrasound principles and interpretation

Nuclear medicine imaging

Angiography techniques

Contrast studies

Interventional radiology procedures

Emergency imaging protocols

Anatomical variants in imaging

Common radiologic findings in pathology
Practice Questions
10 MCQs for Imaging/Clinical
Sample Questions: Imaging/Clinical
Test your understanding with these related questions
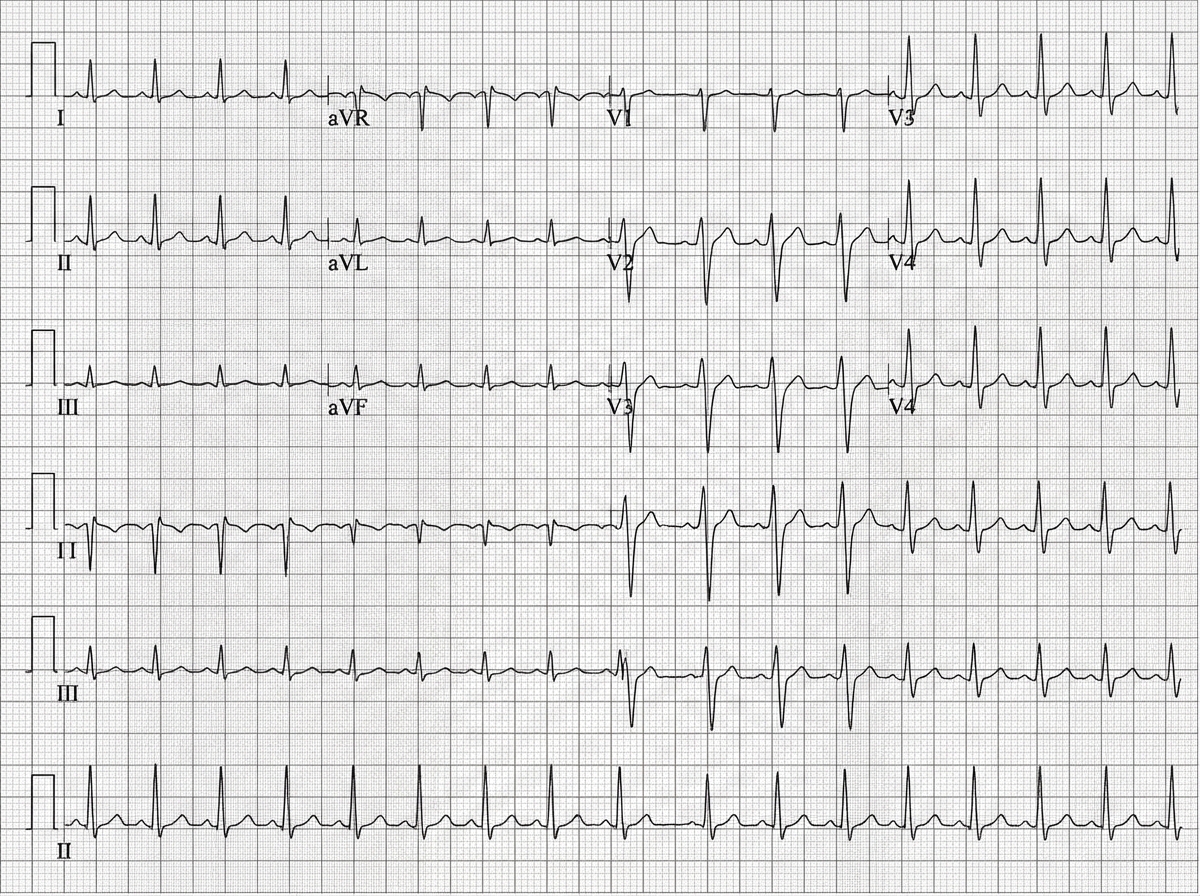
A 45-year-old man is brought to the emergency department after a car accident with pain in the middle of his chest and some shortness of breath. He has sustained injuries to his right arm and leg. He did not lose consciousness. His temperature is 37°C (98.6°F), pulse is 110/min, respirations are 18/min, and blood pressure is 90/60 mm Hg. He is alert and oriented to person, place, and time. Examination shows several injuries to the upper extremities and chest. There are jugular venous pulsations 10 cm above the sternal angle. Heart sounds are faint on cardiac examination. The lungs are clear to auscultation. An ECG is shown. Which of the following is the most appropriate next step in management?
Imaging/Clinical US Medical PG Practice Questions and MCQs
Practice US Medical PG questions for Imaging/Clinical. These multiple choice questions (MCQs) cover important concepts and help you prepare for your exams.
Imaging/Clinical US Medical PG Question 1: A 45-year-old man is brought to the emergency department after a car accident with pain in the middle of his chest and some shortness of breath. He has sustained injuries to his right arm and leg. He did not lose consciousness. His temperature is 37°C (98.6°F), pulse is 110/min, respirations are 18/min, and blood pressure is 90/60 mm Hg. He is alert and oriented to person, place, and time. Examination shows several injuries to the upper extremities and chest. There are jugular venous pulsations 10 cm above the sternal angle. Heart sounds are faint on cardiac examination. The lungs are clear to auscultation. An ECG is shown. Which of the following is the most appropriate next step in management?
- A. Contrast-enhanced CT angiography
- B. Transthoracic echocardiography (Correct Answer)
- C. X-ray of the chest
- D. CT scan of the brain
- E. Contrast esophagram with gastrografin
Imaging/Clinical Explanation: ***Transthoracic echocardiography*** - The patient's presentation with **chest pain**, shortness of breath, **hypotension**, **elevated jugular venous pressure (JVP)**, and **faint heart sounds** after trauma strongly suggests **Beck's triad**, which is classic for **cardiac tamponade**. - **Transthoracic echocardiography** is the fastest and most accurate method to diagnose cardiac tamponade by visualizing pericardial fluid and its hemodynamic effects. *Contrast-enhanced CT angiography* - While CT angiography can detect vascular injuries or aortic dissection, it is not the initial diagnostic test for suspected cardiac tamponade. - The patient's **hemodynamic instability** requires a rapid diagnostic tool to identify life-threatening conditions like tamponade. *X-ray of the chest* - A chest X-ray might show a **widened mediastinum** or **cardiomegaly** if there's a large effusion, but it is not sensitive enough to detect smaller effusions causing tamponade or to assess their hemodynamic impact. - It does not provide real-time visualization of the heart and pericardium, which is crucial in this emergent setting. *CT scan of the brain* - A CT scan of the brain is indicated for suspected head injuries or neurological deficits, but the patient is alert and oriented, and his immediate life threat is clearly thoracic. - Addressing the signs of cardiac tamponade takes precedence over evaluating the brain given his stable neurological status. *Contrast esophagram with gastrografin* - This study is used to diagnose **esophageal perforations**. While possible in significant trauma, the patient's symptoms of **Beck's triad** point specifically to cardiac tamponade, making esophageal perforation a less likely primary diagnosis and this investigation less urgent. - It would not address the immediate, life-threatening cardiovascular compromise.
Imaging/Clinical US Medical PG Question 2: An otherwise healthy 62-year-old woman comes to the physician because of a 3-year history of hearing loss. To test her hearing, the physician performs two tests. First, a vibrating tuning fork is held against the mastoid bone of the patient and then near her ear, to which the patient responds she hears the sound better on both sides when the tuning fork is held near her ear. Next, the physician holds the tuning fork against the bridge of her forehead, to which the patient responds she hears the sound better on the right side than the left. The patient's examination findings are most consistent with which of the following conditions?
- A. Otosclerosis on the left
- B. Cerumen impaction on the right
- C. Cholesteatoma on the right
- D. Acoustic neuroma on the left (Correct Answer)
- E. Cochlear ischemia on the right
Imaging/Clinical Explanation: ***Acoustic neuroma on the left*** - The patient's **Weber test lateralizing to the right** means sound is heard better on the right, indicating either a **sensorineural hearing loss on the left** or a conductive hearing loss on the right. - Her **Rinne test being positive bilaterally** (air conduction > bone conduction) rules out a conductive loss on the right, thus confirming unilateral **sensorineural hearing loss on the left side**. An acoustic neuroma is a common cause of progressive unilateral sensorineural hearing loss. *Otosclerosis on the left* - Otosclerosis typically causes a **conductive hearing loss** due to abnormal bone growth in the middle ear. - A conductive hearing loss on the left would result in the **Weber test lateralizing to the left**, not the right. *Cerumen impaction on the right* - Cerumen impaction causes **conductive hearing loss** in the affected ear. - If the right ear had a conductive loss, the **Weber test would lateralize to the right**, but the Rinne test in the right ear would show bone conduction > air conduction (negative Rinne), which is not the case here. *Cholesteatoma on the right* - A cholesteatoma typically causes **conductive hearing loss** by eroding ossicles or filling the middle ear space. - Similar to cerumen impaction, a conductive loss on the right would lead to a **negative Rinne test on the right**, which is not seen here as the Rinne test is positive bilaterally. *Cochlear ischemia on the right* - Cochlear ischemia would cause **sensorineural hearing loss** in the right ear. - If the right ear had a sensorineural loss, the **Weber test would lateralize to the left**, as the better (left) ear would perceive the sound more clearly, not the right.
Imaging/Clinical US Medical PG Question 3: A 67-year-old man with type 2 diabetes mellitus comes to the emergency department because of lightheadedness over the past 2 hours. He reports that he has had similar episodes of lightheadedness and palpitations over the past 3 days. His only medication is metformin. His pulse is 110/min and irregularly irregular. An ECG shows a variable R-R interval and absence of P waves. The patient undergoes transesophageal echocardiography. During the procedure, the tip of the ultrasound probe is angled posteriorly within the esophagus. This view is most helpful for evaluating which of the following conditions?
- A. Myxoma in the left atrium
- B. Thrombus in the left pulmonary artery
- C. Thrombus in the left ventricular apex
- D. Tumor in the right main bronchus
- E. Aneurysm of the descending aorta (Correct Answer)
Imaging/Clinical Explanation: ***Aneurysm of the descending aorta*** - When the TEE probe is angled **posteriorly within the esophagus**, it optimally visualizes structures directly posterior to the esophagus, particularly the **descending thoracic aorta**. - The descending aorta runs parallel and immediately posterior to the esophagus, making this the ideal view for evaluating **aortic aneurysms, dissections, and atherosclerotic disease** of the descending aorta. - Note: This patient's symptoms (lightheadedness, palpitations) are due to **atrial fibrillation** (irregularly irregular rhythm, absent P waves). The TEE is likely being performed for stroke risk evaluation, but this question tests knowledge of TEE probe positioning and anatomical visualization. *Myxoma in the left atrium* - The left atrium is best visualized using **mid-esophageal views** (especially the 4-chamber view at 0-20 degrees), not a posteriorly angled view. - While TEE is excellent for detecting left atrial myxomas and is commonly performed in AFib patients to evaluate for left atrial appendage thrombus, the posterior angle is not optimal for this structure. *Thrombus in the left pulmonary artery* - The pulmonary arteries are located **anterior** to the esophagus, making them poorly visualized with a posteriorly angled probe. - Pulmonary artery evaluation requires **anterior or superior angulation** of the TEE probe, or CT pulmonary angiography is preferred for pulmonary embolism diagnosis. *Thrombus in the left ventricular apex* - The left ventricular apex is best visualized using **transgastric views** (probe in stomach looking upward), not posterior esophageal views. - LV apex thrombus evaluation requires short-axis and 2-chamber transgastric views at 0-90 degrees. *Tumor in the right main bronchus* - The bronchi are **anterior** to the esophagus and are not adequately visualized with TEE, regardless of probe angle. - TEE is designed for cardiac and great vessel evaluation, not airway pathology; bronchoscopy or CT chest would be appropriate for bronchial tumors.
Imaging/Clinical US Medical PG Question 4: A healthy 22-year-old male participates in a research study you are leading to compare the properties of skeletal and cardiac muscle. You conduct a 3-phased experiment with the participant. In the first phase, you get him to lift up a 2.3 kg (5 lb) weight off a table with his left hand. In the second phase, you get him to do 20 burpees, taking his heart rate to 150/min. In the third phase, you electrically stimulate his gastrocnemius with a frequency of 50 Hz. You are interested in the tension and electrical activity of specific muscles as follows: Biceps in phase 1, cardiac muscle in phase 2, and gastrocnemius in phase 3. What would you expect to be happening in the phases and the respective muscles of interest?
- A. Increase of tension in experiments 2 and 3, with the same underlying mechanism
- B. Increase of tension in all phases (Correct Answer)
- C. Recruitment of large motor units followed by small motor units in experiment 1
- D. Fused tetanic contraction at the end of all three experiments
- E. Recruitment of small motor units at the start of experiments 1 and 2
Imaging/Clinical Explanation: ***Increase of tension in all phases*** - In **phase 1**, lifting a 2.3 kg weight requires the **biceps** to contract, generating sufficient force (**tension**) to overcome gravity. - In **phase 2**, the **cardiac muscle** increases its contractile force (**tension**) to meet the metabolic demands of **exercise**, leading to a heart rate of 150/min. - In **phase 3**, electrical stimulation of the **gastrocnemius** at 50 Hz triggers muscle contraction, leading to an increase in **tension**. *Increase of tension in experiments 2 and 3, with the same underlying mechanism* - While tension increases in phases 2 and 3, the **underlying mechanisms differ**: cardiac muscle tension increases due to increased sympathetic stimulation and preload, while skeletal muscle tension increases due to unfused or fused tetanus from electrical stimulation. - Cardiac muscle contraction is regulated by **calcium-induced calcium release**, while skeletal muscle involves direct coupling of DHP receptor and ryanodine receptor. *Recruitment of large motor units followed by small motor units in experiment 1* - **Motor unit recruitment** follows the **size principle**, meaning smaller, more easily excitable motor units are activated first, followed by larger ones as more force is needed. - Therefore, in phase 1, **small motor units** would be recruited first, not large ones. *Fused tetanic contraction at the end of all three experiments* - **Fused tetanic contraction** occurs in **skeletal muscle** when stimulation frequency is high enough that individual twitches summate completely, leading to sustained contraction. - This phenomenon is **not possible in cardiac muscle** due to its long **refractory period**, which prevents sustained contraction and allows for adequate filling time. *Recruitment of small motor units at the start of experiments 1 and 2* - **Motor unit recruitment** applies to **skeletal muscle** (phase 1) and involves recruiting small motor units first for fine or gentle movements. - **Cardiac muscle** (phase 2) does not have motor units; instead, it relies on the **Frank-Starling mechanism** and hormonal/nervous regulation to adjust its contractile force as a syncytium.
Imaging/Clinical US Medical PG Question 5: A 27-year old primigravid woman at 37 weeks' gestation comes to the emergency department because of frequent contractions for 4 hours. Her pregnancy has been complicated by hyperemesis gravidarum which subsided in the second trimester. The contractions occur every 10–15 minutes and have been increasing in intensity and duration since onset. Her temperature is 37.1°C (98.8°F), pulse is 110/min, and blood pressure is 140/85 mm Hg. Uterine contractions are felt on palpation. Pelvic examination shows clear fluid in the vagina. The cervix is 50% effaced and 3 cm dilated. After 4 hours the cervix is 80% effaced and 6 cm dilated. Pelvic examination is inconclusive for the position of the fetal head. The fetal heart rate is reassuring. Which of the following is the most appropriate next step?
- A. Administer oxytocin
- B. Perform external cephalic version
- C. Administer misoprostol
- D. Perform Mauriceau-Smellie-Veit maneuver
- E. Perform ultrasonography (Correct Answer)
Imaging/Clinical Explanation: ***Perform ultrasonography*** - The examination notes that the **pelvic examination is inconclusive for the position of the fetal head**, which is a critical piece of information needed for safe delivery. **Ultrasonography** is the most appropriate next step to ascertain the fetal presentation and position, especially given the dilated cervix. - Determining fetal position is essential to rule out **malpresentation**, such as **breech** or **transverse lie**, which would significantly impact the delivery plan and potentially necessitate a **cesarean section**. *Administer oxytocin* - **Oxytocin** is used to induce or augment labor when contractions are insufficient or labor is prolonged, but in this case, the cervix is progressing well (from 3 cm to 6 cm dilation in 4 hours), indicating **active labor**. - Without knowing the fetal presentation, administering oxytocin could exacerbate issues if there's a **malpresentation**, potentially leading to **fetal distress** or **uterine rupture**. *Perform external cephalic version* - **External cephalic version (ECV)** is performed to change a **breech presentation** to a **cephalic presentation** by external manipulation, typically done before labor onset or early in labor at term. - This patient is already in **active labor** with significant cervical dilation (6 cm), making ECV less likely to be successful and potentially increasing risks like **placental abruption** or **umbilical cord compression**. *Administer misoprostol* - **Misoprostol** is a prostaglandin analog used for **cervical ripening** and **labor induction** in cases where the cervix is unfavorable or labor needs to be initiated. - This patient is already in **active labor** with progressive cervical dilation, making misoprostol unnecessary and potentially harmful due to the risk of **uterine hyperstimulation**. *Perform Mauriceau-Smellie-Veit maneuver* - The **Mauriceau-Smellie-Veit maneuver** is a technique used during a **vaginal breech delivery** to deliver the fetal head, specifically in cases of **frank or complete breech** that are being delivered vaginally. - This maneuver is only performed *during* delivery of a breech baby, and the fetal position is currently unknown. It would be premature and inappropriate to consider this maneuver without first confirming a **breech presentation** and the decision for vaginal delivery.
More Imaging/Clinical US Medical PG questions available in the OnCourse app. Practice MCQs, flashcards, and get detailed explanations.
Flashcards
10 cards for Imaging/Clinical
Sample Flashcards: Imaging/Clinical
In portal hypertension, the _____ vein backs up into the esophageal vein, resulting in varices
In portal hypertension, the _____ vein backs up into the esophageal vein, resulting in varices
left gastric
Imaging/Clinical Flashcards - Medical Study Cards by OnCourse
Master Imaging/Clinical with OnCourse flashcards. These spaced repetition flashcards are designed for medical students preparing for NEET PG, USMLE Step 1, USMLE Step 2, MBBS exams, and other medical licensing examinations.
OnCourse flashcards use active recall and spaced repetition techniques similar to Anki to help you memorize and retain medical concepts effectively. Each card is crafted by medical experts to cover high-yield topics.
Why use OnCourse Flashcards for Imaging/Clinical?
- Spaced repetition algorithm for optimal retention
- Anki-style cloze deletions for active recall
- Created by medical professionals and educators
- Covers NEET PG, USMLE, PLAB, and MBBS curricula
- Mobile app available for studying on the go
Imaging/Clinical Flashcard Deck - 5 Cards
Imaging/Clinical Flashcard 1 of 5
Question: In portal hypertension, the _____ vein backs up into the esophageal vein, resulting in varices
Answer: left gastric
Imaging/Clinical Flashcard 2 of 5
Question: _____ is a congenital lung malformation that presents as discrete, round, sharply defined and air-filled densities on CXR
Answer: Bronchogenic cyst
Imaging/Clinical Flashcard 3 of 5
Question: Thrombosis most commonly occurs in the _____ of the leg below the knee
Answer: deep veins (DVT)
Imaging/Clinical Flashcard 4 of 5
Question: Enlargement of the heart can cause _____ due to compression of the left recurrent laryngeal nerve
Answer: hoarseness
Imaging/Clinical Flashcard 5 of 5
Question: Congenital adrenal hyperplasia affects the adrenal glands on _____ side(s) of the body (one or both)
Answer: both
Download the OnCourse app to access all 5 flashcards for Imaging/Clinical, plus thousands more covering Anatomy, Physiology, Pathology, Pharmacology, Microbiology, Biochemistry, and all medical subjects. Better than Anki for medical students!
Keywords: Imaging/Clinical flashcards, medical flashcards, NEET PG preparation, USMLE Step 1 flashcards, Anki alternative, spaced repetition medical, OnCourse flashcards, medical exam preparation, MBBS study material, active recall medical education
Have doubts about this lesson?
Ask Rezzy, our AI tutor, to explain anything you didn't understand
About Imaging/Clinical for USMLE
Imaging/Clinical is a key topic within Anatomy for USMLE preparation. OnCourse provides 11 comprehensive lessons, 10 practice MCQs, and 10 flashcards to help you master this topic.
Lessons in Imaging/Clinical
- X-ray principles and interpretation
- CT scan principles and interpretation
- MRI principles and interpretation
- Ultrasound principles and interpretation
- Nuclear medicine imaging
- Angiography techniques
- Contrast studies
- Interventional radiology procedures
- Emergency imaging protocols
- Anatomical variants in imaging
- Common radiologic findings in pathology
Part of Anatomy for USMLE preparation on OnCourse.
Master Imaging/Clinical
Get full access to all 11 lessons, 10 questions, and AI-powered study tools.
Start For Free