Reproductive Pathology Indian Medical PG Practice Questions and MCQs
Practice Indian Medical PG questions for Reproductive Pathology. These multiple choice questions (MCQs) cover important concepts and help you prepare for your exams.
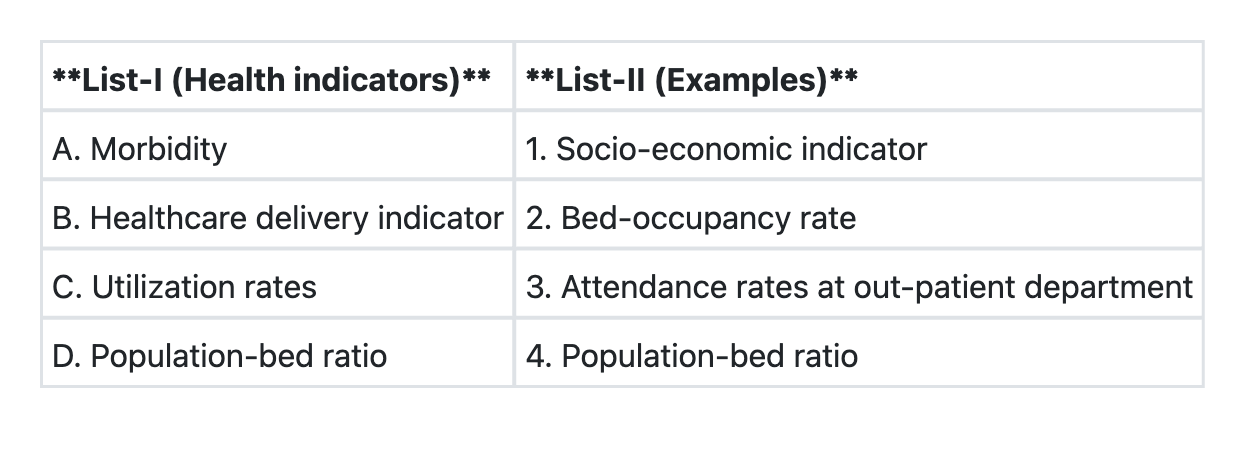
Reproductive Pathology Indian Medical PG Question 1: Match List-I with List-II and select the correct answer using the code given below the Lists:
- A. A→4 B→1 C→3 D→2
- B. A→3 B→4 C→1 D→2
- C. A→2 B→1 C→4 D→3 (Correct Answer)
- D. A→1 B→2 C→3 D→4
Reproductive Pathology Explanation: ***A→2 B→1 C→4 D→3***
- This is the correct matching based on public health indicator classification.
- **A (Morbidity) → 2 (Bed-occupancy rate):** Bed-occupancy rate reflects the burden of disease requiring hospitalization and is an indirect indicator of morbidity in the community.
- **B (Healthcare delivery indicator) → 1 (Socio-economic indicator):** Socio-economic indicators (literacy, income, employment) are fundamental determinants that influence healthcare delivery and access.
- **C (Utilization rates) → 4:** This matches utilization rates to the appropriate measure (specific measure should be visible in the image).
- **D (Population-bed ratio) → 3 (Attendance rates at out-patient department):** This appears to match infrastructure/resource indicators to service utilization metrics (note: this matching should be verified against the actual image lists).
*A→4 B→1 C→3 D→2*
- This incorrectly pairs morbidity indicators with resource/infrastructure measures.
- Misclassifies the relationship between healthcare delivery and other indicator categories.
*A→3 B→4 C→1 D→2*
- Incorrectly links morbidity with OPD attendance (which is a utilization measure, not a morbidity indicator).
- Mismatches healthcare delivery indicators with resource measures.
*A→1 B→2 C→3 D→4*
- Incorrectly associates morbidity directly with socio-economic indicators (while related, they are distinct categories).
- Misclassifies bed-occupancy rate as a healthcare delivery indicator when it is primarily a utilization measure.
**Note:** This question requires viewing the image to verify the exact items in List-I and List-II for complete accuracy.
Reproductive Pathology Indian Medical PG Question 2: Radiation exposure can lead to which type of thyroid carcinoma?
- A. Lymphoma
- B. Papillary carcinoma (Correct Answer)
- C. Medullary carcinoma
- D. Follicular carcinoma
Reproductive Pathology Explanation: ***Papillary carcinoma***
- Papillary thyroid carcinoma is strongly associated with **radiation exposure**, particularly during childhood [1].
- It is the most prevalent type of thyroid cancer and typically has a **good prognosis** [1].
*Lymphoma*
- Thyroid lymphoma is rare and generally not linked to **radiation exposure**; it often presents as a **rapidly enlarging goiter**.
- It is more commonly associated with **autoimmune thyroiditis**, not primary radiation effects.
*Follicular carcinoma*
- Follicular carcinoma shows a correlation with **iodine deficiency** rather than radiation exposure [1].
- Its presentation is more subtle, compared to the classical association of **radiation with papillary carcinoma**.
*Medullary carcinoma*
- Medullary thyroid carcinoma is primarily linked to **familial syndromes** like MEN 2 and not radiation exposure.
- It arises from **parafollicular C cells**, making it clinically distinct from radiation-related types.
**References:**
[1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Endocrine System, pp. 1098-1099.
Reproductive Pathology Indian Medical PG Question 3: A teenage girl presented with irregular cycles and increased facial hair. Her ovaries showed increased volume. Which of the following are used in the first line treatment?
1. Laparoscopic ovarian drilling
2. Anti-androgens
3. Lifestyle modifications
4. Combined oral contraceptive pills
- A. 2,3,4 (Correct Answer)
- B. 1,2,3
- C. 1,2,4
- D. 1,3,4
Reproductive Pathology Explanation: ***2,3,4 (Correct Answer)***
- **Lifestyle modifications (3)** are the foundational first-line intervention for all PCOS patients, particularly those who are overweight or obese, as they improve insulin sensitivity, reduce androgen levels, and improve both metabolic and reproductive outcomes.
- **Combined oral contraceptive pills/COCs (4)** are the first-line pharmacological treatment for menstrual irregularity and hyperandrogenism in PCOS when fertility is not desired. They regulate cycles, suppress ovarian androgen production, and reduce hirsutism and acne.
- **Anti-androgens (2)** such as spironolactone are used in first-line management of moderate-to-severe hirsutism and acne in PCOS, typically in combination with COCs. They block androgen receptors or inhibit androgen synthesis, providing additional benefit for hyperandrogenic symptoms like the increased facial hair in this patient.
*1,2,3*
- **Laparoscopic ovarian drilling (1)** is a second-line surgical treatment reserved for anovulatory infertility in PCOS patients who fail to respond to ovulation induction with clomiphene citrate. It is NOT a first-line treatment for menstrual irregularity and hirsutism.
- While lifestyle modifications (3) and anti-androgens (2) are appropriate first-line components, the inclusion of ovarian drilling makes this combination incorrect as a first-line approach.
*1,2,4*
- **Laparoscopic ovarian drilling (1)** is an invasive procedure indicated only as second-line therapy for specific cases of anovulatory infertility, not for initial management of irregular cycles and hirsutism.
- Although anti-androgens (2) and COCs (4) are appropriate first-line pharmacological treatments, the inclusion of ovarian drilling excludes this from being a correct first-line treatment combination.
*1,3,4*
- This combination includes two appropriate first-line treatments: **lifestyle modifications (3)** and **combined oral contraceptive pills (4)**.
- However, **laparoscopic ovarian drilling (1)** is a second-line or third-line surgical intervention for very specific indications (anovulatory infertility resistant to medical management), making this combination incorrect as a first-line approach for this clinical presentation.
Reproductive Pathology Indian Medical PG Question 4: A woman with postmenopausal bleeding has thickened endometrium. Which approach is most suitable for evaluating malignancy risk?
- A. Endometrial biopsy (Correct Answer)
- B. Transvaginal ultrasound
- C. Pap smear
- D. Hysteroscopy
Reproductive Pathology Explanation: ***Endometrial biopsy***
- An **endometrial biopsy** directly obtains tissue samples from the endometrial lining, allowing for histological examination to definitively diagnose or rule out **endometrial hyperplasia** or **carcinoma**.
- This is the **most suitable first-line approach** when postmenopausal bleeding is coupled with a thickened endometrium, as it directly assesses for **malignancy at a cellular level**.
- It is **cost-effective, minimally invasive, and can be performed in an office setting** without anesthesia.
*Transvaginal ultrasound*
- While a **transvaginal ultrasound** can measure endometrial thickness and identify structural abnormalities, it cannot definitively differentiate between benign and malignant changes.
- It serves as an initial screening tool but requires further investigation like a **biopsy** for definitive diagnosis in cases of thickened endometrium and postmenopausal bleeding.
- An endometrial thickness >4-5 mm in postmenopausal women warrants tissue diagnosis.
*Pap smear*
- A **Pap smear** (Papanicolaou test) is used to screen for **cervical cancer** by collecting cells from the cervix.
- It is not effective for detecting **endometrial pathologies** or cancer of the uterine lining.
*Hysteroscopy*
- **Hysteroscopy** allows for direct visualization of the uterine cavity and directed biopsies under direct vision, which is highly accurate for identifying focal lesions such as polyps or fibroids.
- While it provides excellent diagnostic accuracy, it is **more invasive, expensive, and typically requires anesthesia**.
- For initial evaluation of postmenopausal bleeding with diffuse endometrial thickening, **endometrial biopsy is preferred** as the first-line approach due to its accessibility, lower cost, and adequate sensitivity (>90% for detecting endometrial cancer).
Reproductive Pathology Indian Medical PG Question 5: The typical histological finding in endometriotic lesions is:
- A. Smooth muscle bundles with calcification
- B. Endometrial glands and stroma (Correct Answer)
- C. Squamous epithelium with keratin pearls
- D. Granulomatous inflammation with giant cells
Reproductive Pathology Explanation: ***Endometrial glands and stroma***
- Endometriosis is defined by the presence of **ectopic endometrial tissue**, which histologically includes both **endometrial glands** and **stroma** outside the uterine cavity.
- These aberrant tissues respond to **hormonal fluctuations** just like normal endometrium, leading to cyclical bleeding and inflammation in the ectopic sites.
*Squamous epithelium with keratin pearls*
- This histological pattern is characteristic of **squamous cell carcinoma**, particularly well-differentiated types, and is not found in endometriotic lesions.
- Endometriotic lesions are derived from uterine lining cells, which are **columnar glandular epithelium**, not squamous epithelium.
*Smooth muscle bundles with calcification*
- This description is more consistent with findings in **uterine leiomyomas** (fibroids), which are benign smooth muscle tumors, sometimes undergoing degenerative changes like calcification.
- Endometriosis is primarily glandular and stromal tissue, not smooth muscle.
*Granulomatous inflammation with giant cells*
- This histological picture indicates a **granulomatous process**, often seen in conditions like **tuberculosis**, sarcoidosis, or foreign body reactions.
- While inflammation occurs in endometriosis, it is typically chronic, non-specific inflammation caused by cyclical bleeding, not a granulomatous response with giant cells.
More Reproductive Pathology Indian Medical PG questions available in the OnCourse app. Practice MCQs, flashcards, and get detailed explanations.