Urinary stones: types, CT KUB findings and management pathway
Ah, the dreaded kidney stone! Probably the closest a man can get to labor pains, or so they say. Since you're prepping for the UKMLA AKT, this is a classic "bread and butter" topic that you'll definitely see in some form.
Let's start with the different "flavors" of stones you might encounter. I've put together a quick comparison table to help you distinguish them, especially which ones are radio-opaque versus radiolucent.
| Stone Type | Frequency | Characteristics | Radiopacity |
|---|---|---|---|
| Calcium Oxalate | ~80% | Most common; associated with hypercalciuria, hyperoxaluria. | Radio-opaque |
| Calcium Phosphate | ~10% | Often seen in Renal Tubular Acidosis (Type 1) or hyperparathyroidism. | Radio-opaque |
| Struvite (Triple Phosphate) | ~10% | "Staghorn" calculi; associated with urease-producing bacteria (e.g., Proteus mirabilis). | Radio-opaque |
| Uric Acid | ~5% | Associated with gout and high cell turnover (leukemia); acidic urine. | Radiolucent (Invisible on X-ray!) |
| Cystine | <1% | Inherited (cystinuria); "hexagonal" crystals on microscopy. | Semi-opaque ("Ground glass") |
When you're suspecting a stone, the Non-contrast CT KUB (NCCT) is the gold standard investigation. It's fast, highly sensitive, and doesn't require contrast, which is great because contrast can actually mask the stone!
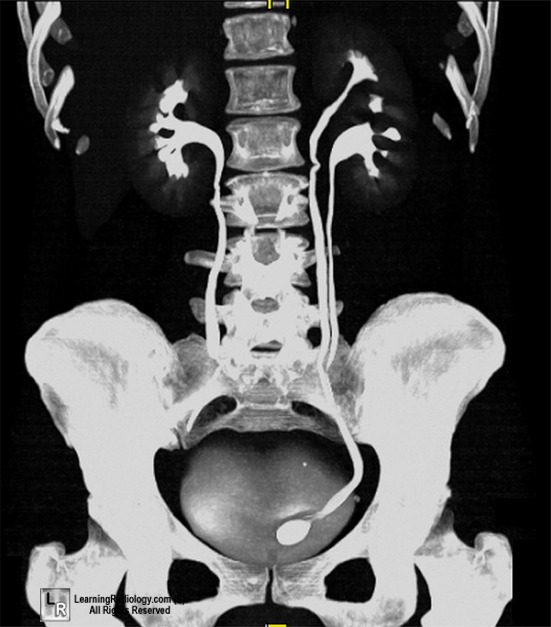
I'll find a good image to show you what a stone looks like on a CT scan. Pay attention to the "rim sign" — it's a classic finding where the ureteral wall is thickened around the stone.
Here's a great example of what a stone looks like on a CT scan. You can see the dilation of the ureter (hydroureter) above the obstructing stone.
When it comes to management, the size and location of the stone, along with any signs of infection, dictate the pathway. In the UK, we follow NICE guidelines, which emphasize NSAIDs (like Diclofenac or Ibuprofen) as the first-line analgesia — they're actually more effective than opioids for renal colic!
Here's a simplified management pathway for you.
I'll also pull up some lessons so you can dive deeper into the pathophysiology and long-term prevention. It's high-yield to know about the metabolic workup (like 24-hour urine collection) for recurrent stone formers!
📚 Urinary Stone Lessons
Those lessons should give you a solid foundation! Just a couple of final high-yield nuggets for your AKT:
- The "Rim Sign": On CT, this is the soft-tissue "halo" around the stone caused by ureteral wall edema. It helps distinguish a stone from a phlebolith (calcified pelvic vein), which doesn't have a rim.
- Staghorn Calculi: These are almost always Struvite (Triple Phosphate) and are caused by urease-producing bugs like Proteus. They thrive in alkaline urine.
- Uric Acid Stones: These are the "stealth" stones—they don't show up on X-ray (radiolucent) but are clearly visible on CT. They're associated with acidic urine.
- Emergency Decompression: If a patient has a stone AND signs of infection (fever, high WCC), that's a surgical emergency. You must decompress the system with a nephrostomy or stent immediately to prevent urosepsis.
Do you want to try a quick case study to see how you'd manage a patient in the ED, or should we look at some flashcards for the stone types?
Setting up chat...